
The Extended Lateral Approach to the Calcaneus – The Large L-Shaped Incision
1.Overview
The extended lateral approach to the calcaneus is the most commonly used surgical approach for treating displaced intra‑articular calcaneal fractures. Over 90% of calcaneal fractures with articular displacement can be managed through this approach.
Although calcaneal fractures vary considerably in morphology, this approach remains the safest and most practical option when performed with meticulous technique.
2. Anatomical Considerations for Blood Supply
Understanding the blood supply to the subcutaneous tissue of the lateral hindfoot is critical, as wound healing problems are common after this approach. Perforating branches of the peroneal artery provide vascularity to the lateral skin and soft tissue of the foot. Subcutaneous undermining of the skin margin may lead to necrosis; therefore, a full‑thickness flap must be raised to prevent such complications.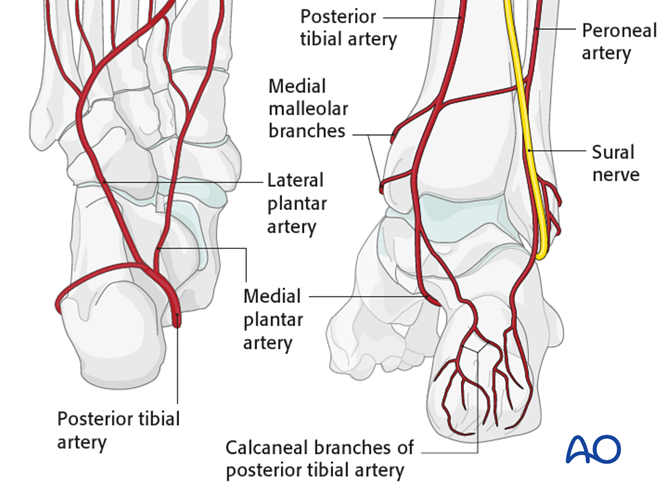
- The lateral calcaneal artery supplies the main blood flow to the corner of this L‑shaped flap.
- The heel pad receives its blood supply primarily from the medial branches of the posterior tibial artery.
- The sural nerve must be protected along the horizontal limb of the incision.
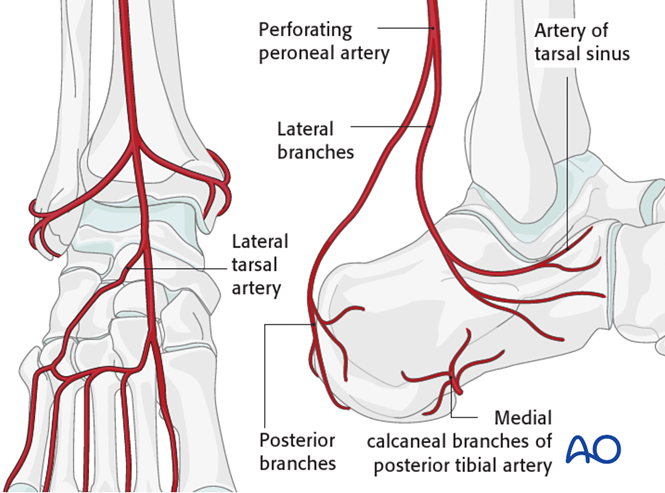
- Artery of the tarsal sinus (a branch of the dorsalis pedis artery distributing to the lateral tarsal region) – supplies the sinus tarsi region (the important anatomical space between the talus and calcaneus).
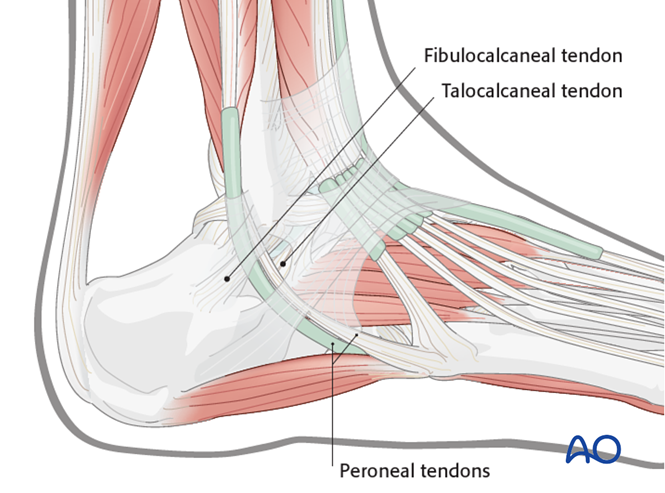
Ligaments and Tendons
The peroneal tendons lie on the lateral aspect of the calcaneus. Attention should be paid to the extensor retinaculum, the calcaneofibular ligament, and the talocalcaneal ligament. When raising the full‑thickness L‑shaped flap, the attachments of the retinaculum, the calcaneofibular ligament, and the talocalcaneal ligament must be stripped off the bone.
3. Surgical Timing
Correct timing of surgery is key to preventing local wound complications. Operating too early increases the risk of skin edge necrosis; patience is required to achieve optimal conditions.
- Observe and protect any skin blisters.
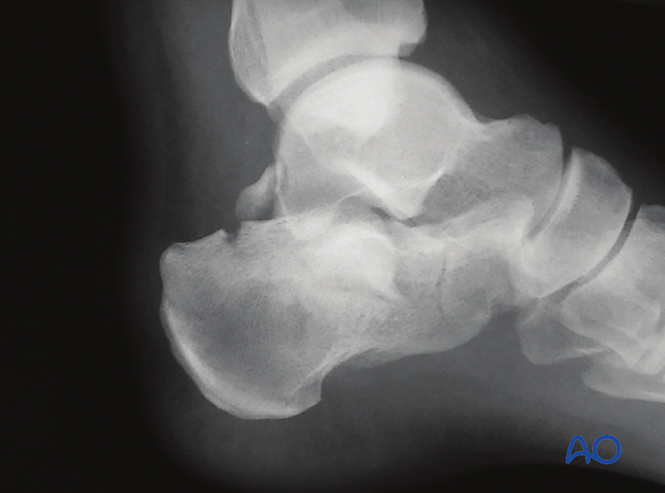
- Image caption: A severely injured foot on day 3 post‑trauma – not yet suitable for surgery.

The return of skin wrinkles over the lateral foot (the "wrinkle sign") is used as the criterion for surgical timing. Generally, the optimal window is 8–14 days after injury. Delaying surgery beyond this period may increase the difficulty of reduction and wound closure.
- Image caption: A foot suitable for surgery at 14 days post‑trauma, showing a clear wrinkle sign.

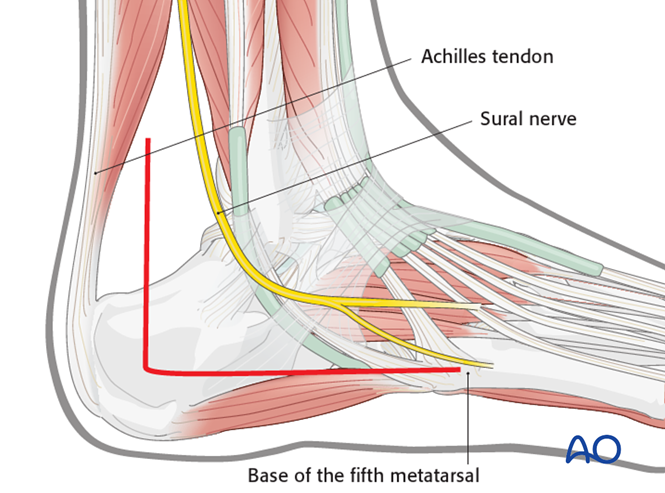
4. Incision and Flap Elevation
The blood supply of the skin incision lies in a "watershed" area. Special attention must be paid to the soft‑tissue flap at the junction of the vertical and horizontal limbs.
- The posterior limb is placed midway between the fibula and the Achilles tendon.
- The horizontal limb follows the base of the fifth metatarsal.
- The skin edges at the corner require meticulous handling.
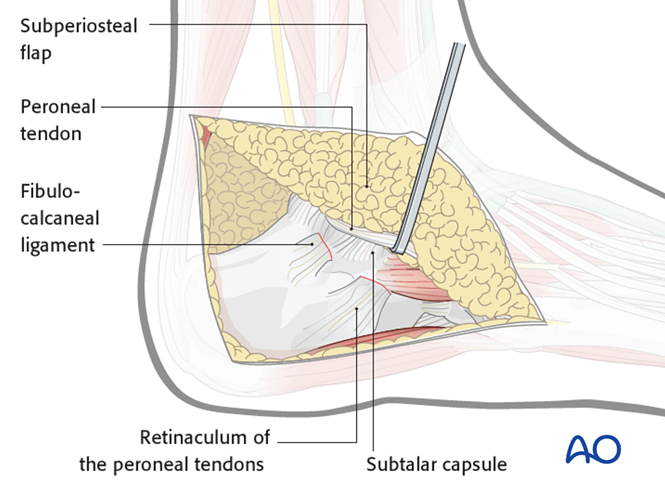
Flap Elevation
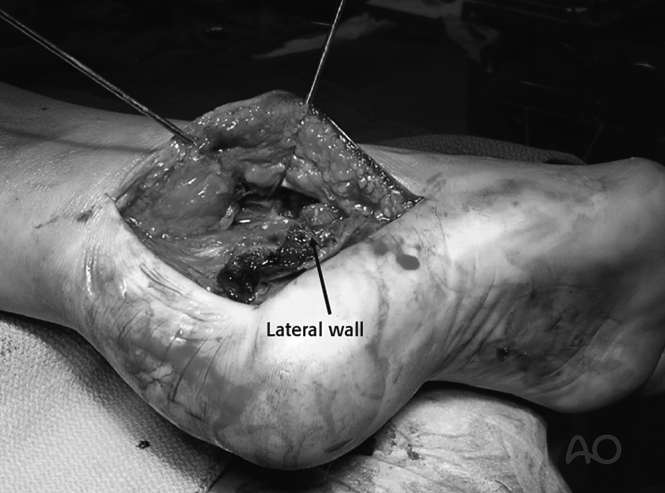
The incision at the corner must be carried down directly to bone to ensure a full‑thickness flap. Avoid subcutaneous undermining. When raising the flap, cut through the retinaculum and strip the calcaneofibular and talocalcaneal ligaments off the bone. The peroneal tendons and the sural nerve are kept within the flap and not exposed. Upward elevation exposes the subtalar joint and the sinus tarsi.
Arthrotomy
Incise the subtalar capsule.
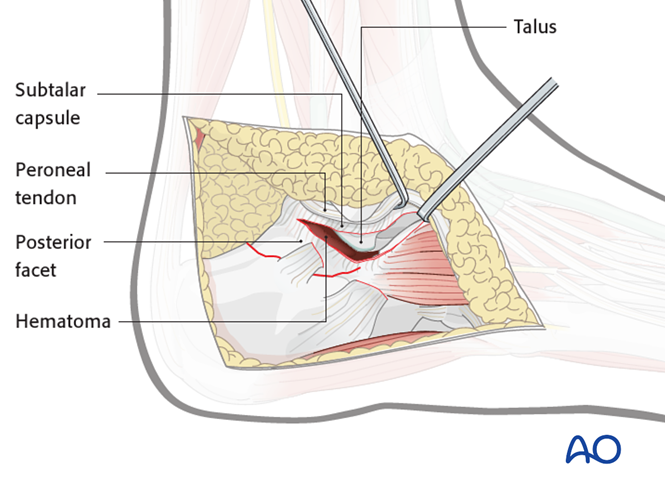
Talus
After evacuating the hematoma, insert Kirschner wires into the lateral process of the talus and the fibula for distraction.
5. Wound Closure
Closed in two layers with negative‑pressure drainage:
- Absorbable sutures for subcutaneous tissue approximation.
- Ensure that the distal corner of the incision is not under excessive tension; advance the flap if necessary.
- Interrupted skin sutures using the **Allgöwer‑Donati** technique, with meticulous edge eversion.

Healing Complications
Wound problems occur in approximately 15% of cases, most commonly affecting the tip of the incision. Manifestations may include skin edge necrosis, soft‑tissue infection, and in severe cases, deep infection. Most can be managed with close observation, antibiotic therapy, wound care, and debridement.