
Minimally Invasive Lateral/Anterolateral MIPO Approach to the Distal Femur
1.Surgical Principles
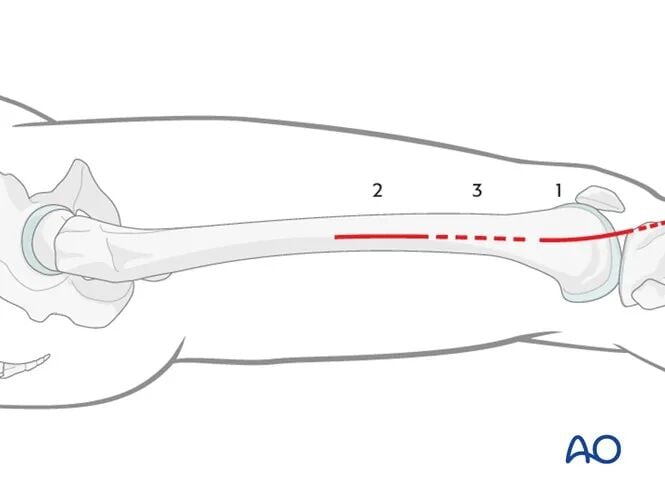
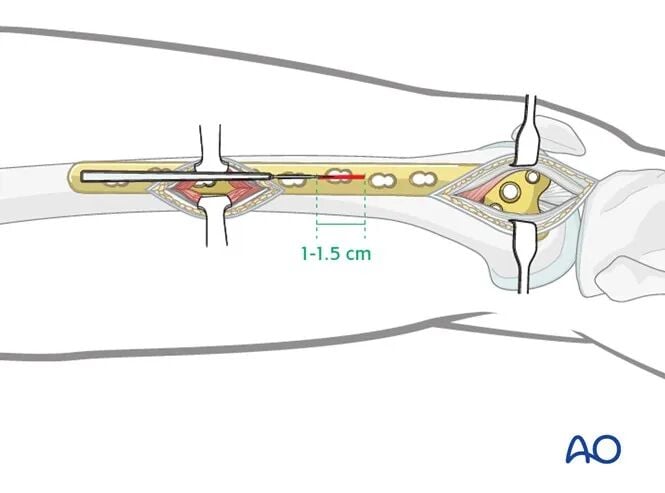
The minimally invasive plate osteosynthesis (MIPO) lateral approach to the femur combines a short version of the lateral incision to the distal femur, a minimally invasive approach to the middle or proximal femoral shaft, and 1.0–1.5 cm stab incisions.
The lateral MIPO approach consists of:
1. A short version of the lateral incision to the distal femur (with or without arthrotomy). Illustrated guide to the lateral/anterolateral approach to the distal femur (AO Surgery Reference).
2. A minimally invasive approach to the middle femoral shaft, allowing the surgeon to ensure proper plate positioning more proximally on the femur.
3. 1.0–1.5 cm stab incisions for percutaneous screw insertion.
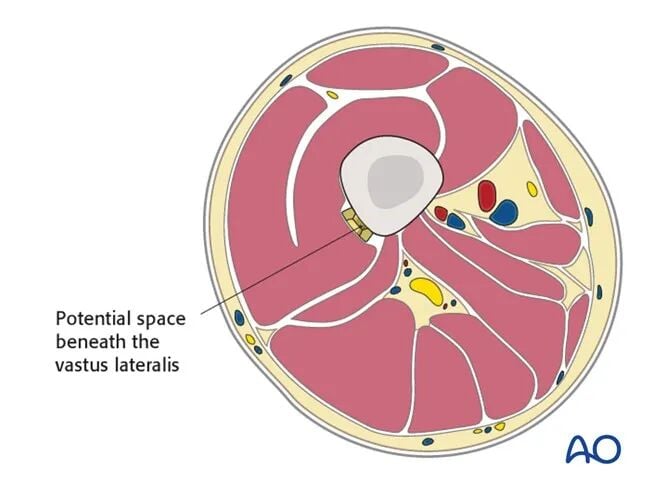
The plate is inserted in a minimally invasive, epiperiosteal manner, gliding within the natural potential space beneath the vastus lateralis muscle.
2. Prophylactic Antibiotics
Antibiotic use should follow local protocols and individual patient requirements. For closed fractures, most surgeons use prophylactic antibiotics covering Gram-positive organisms. For open fractures, additional coverage for Gram-negative organisms is typically added.
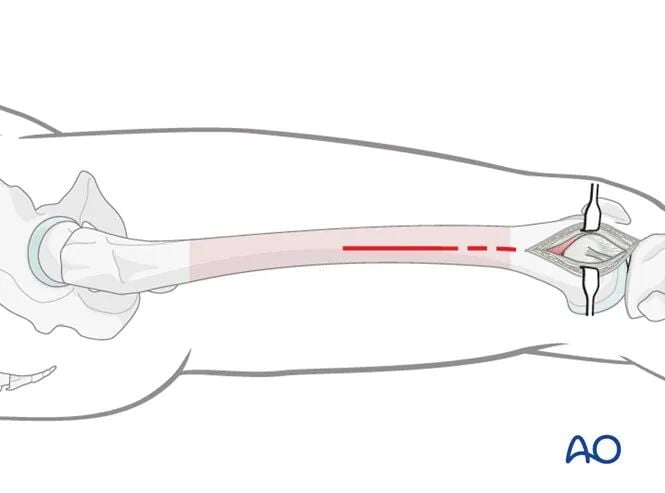
3. Distal Approach (Skin Incision)
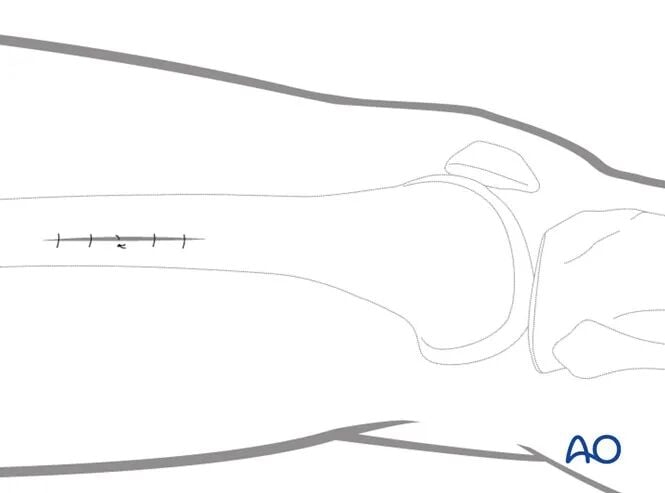
The skin incision for MIPO of distal femoral fractures is simply a shorter version of the standard lateral open approach to the distal femur.
As with the standard lateral open approach, the distal extension of the incision depends on the need for an arthrotomy. However, the proximal extension of the incision is shorter, as the plate will be inserted through an epiperiosteal tunnel.
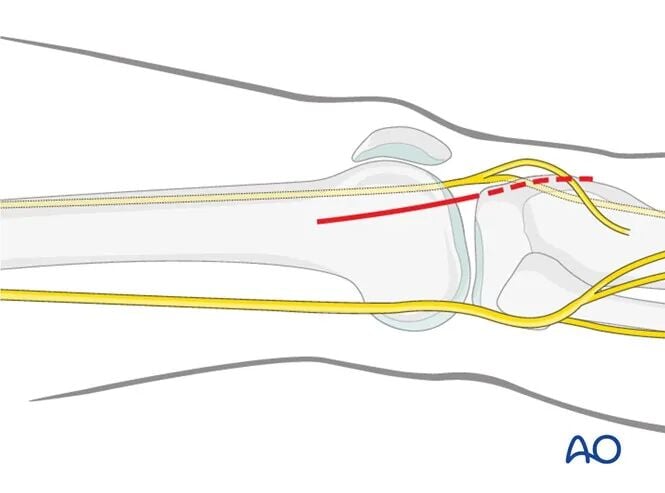
The proximal starting point of the skin incision is at the metaphyseal level of the distal femur. Distal extension of the incision depends on the need for arthrotomy:
* If joint visualization is required, the incision extends to the level of Gerdy's tubercle (dashed line).
* If arthrotomy is not required, the skin incision may terminate approximately 1–2 cm distal to the joint line.
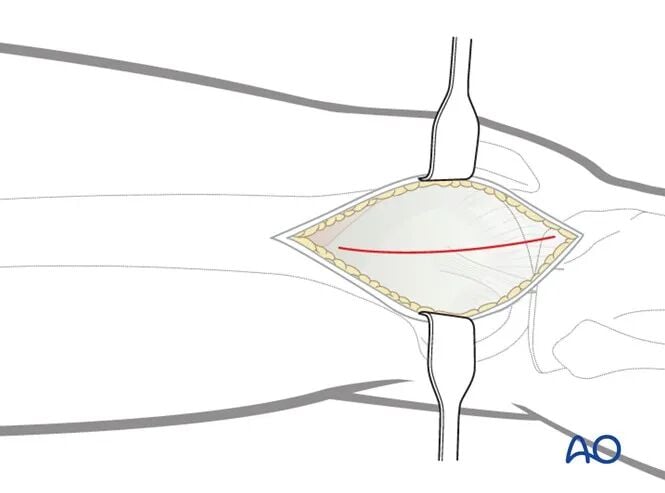
Incision of the Iliotibial Band
The iliotibial (IT) band is incised in line with the skin incision.
Distally, the fibers of the IT band run obliquely anteriorly toward Gerdy's tubercle; the incision should follow the direction of these fibers.
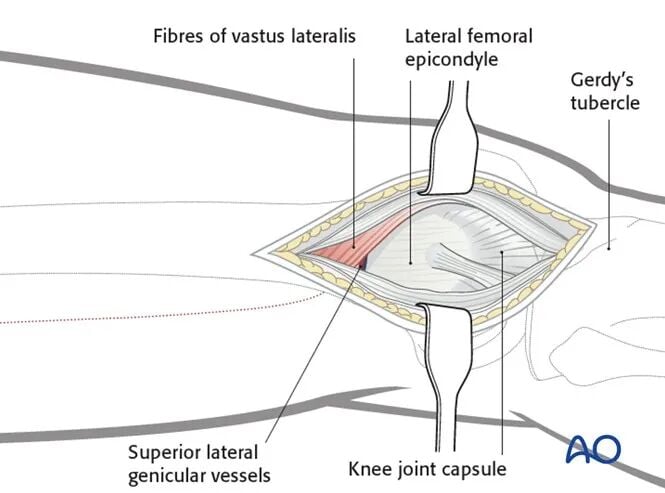
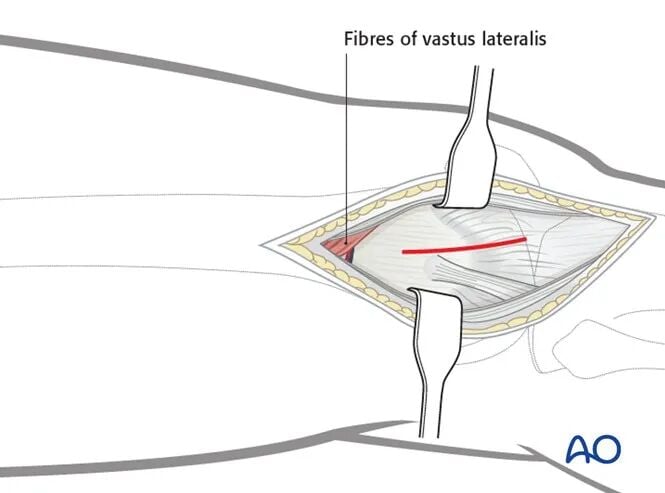
Key Point: Vastus Lateralis Muscle
Unlike the standard lateral approach to the distal femur, the vastus lateralis muscle is largely not elevated in the MIPO approach.
Over the distal 8–10 cm of the femur, the vastus lateralis muscle has very few fibers. Therefore, if no arthrotomy is performed, after incising the IT band, the lateral aspect of the distal femur is readily exposed for minimally invasive fixation.
Branches of the superior lateral genicular artery and vein should be coagulated or ligated as needed.
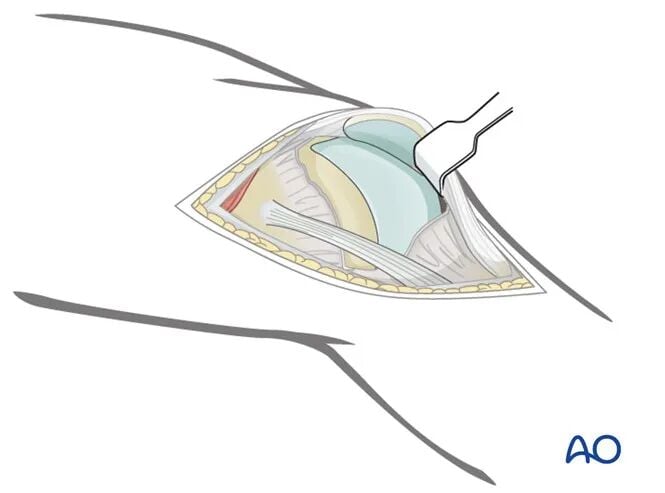
Articular Surface Visualization (Arthrotomy)
If visualization of the articular surface is necessary, an arthrotomy is required. This involves extending the incision distally by approximately 3–4 cm.
Arthrotomy Technique
The arthrotomy is performed by incising the knee joint capsule at the junction of the anterior and middle thirds of the lateral femoral condyle. The incision can be extended distally to the anterior aspect of the lateral meniscus.
A blunt, right-angled retractor can be used to assist in visualizing the articular surface, taking care to avoid excessive traction on the patellar tendon, especially in osteoporotic patients.
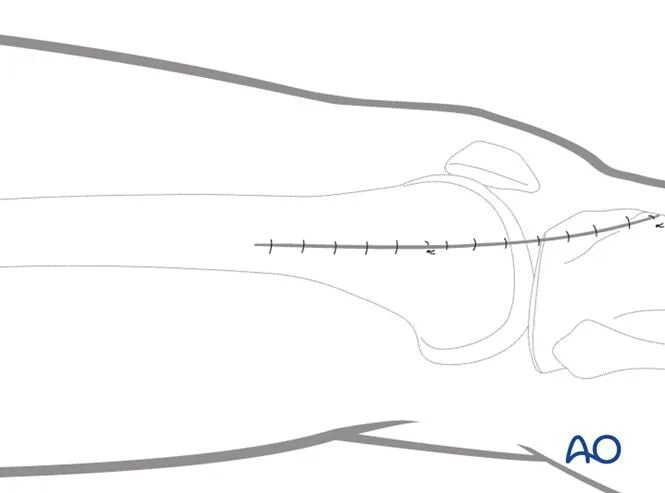
Closure
The arthrotomy incision and the iliotibial band are closed with absorbable sutures. Subcutaneous tissue and skin are closed in standard fashion.
4. Mid-Proximal Femoral Shaft Minimally Invasive Approach
Skin Incision
A short incision is made along the imaginary line connecting the lateral femoral epicondyle and the greater trochanter (dashed line).
The exact starting point and length of the incision are determined by the intraoperative requirements of the minimally invasive procedure.
Approach
The fascia lata is incised to expose the fascia overlying the vastus lateralis muscle. The vastus lateralis fascia is carefully incised.
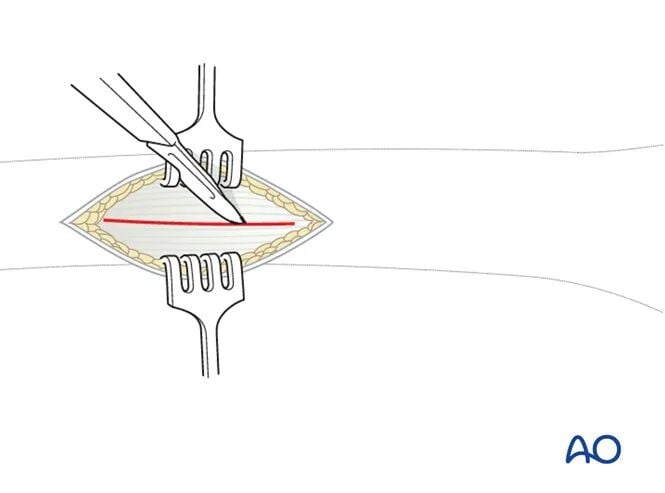
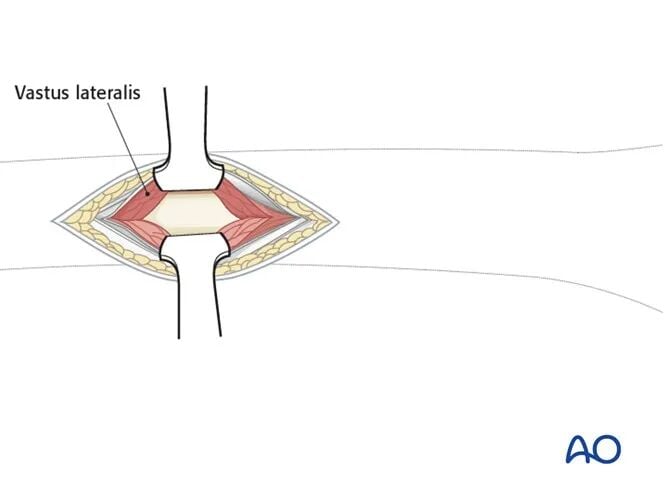
The muscle fibers are bluntly separated down to the femur.
Note: While the standard lateral approach to the femur involves elevating the entire vastus lateralis muscle belly anteriorly off the lateral intermuscular septum, this is not feasible with minimally invasive techniques. Therefore, the muscle belly is split in line with its fibers to expose the lateral femur.
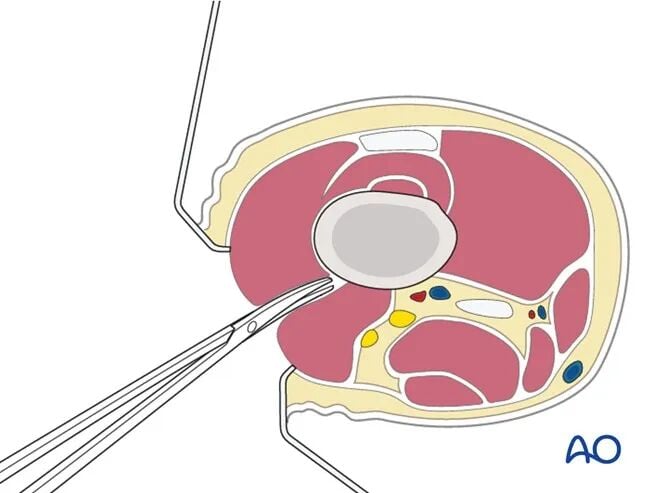
Exposure and Retraction
The use of two Hohmann retractors (one placed anteriorly and one posteriorly) is recommended to provide stable exposure of the femoral shaft.
Hohmann retractors help ensure proper plate positioning on the femur.
It is advisable to confirm that the most proximal screw hole in the plate is centered on the femoral shaft before inserting the remaining proximal screws.
Closure
The iliotibial band is closed with absorbable sutures. Subcutaneous tissue and skin are closed in standard fashion.
5. Percutaneous Screw Insertion (Stab Incisions)
Incision
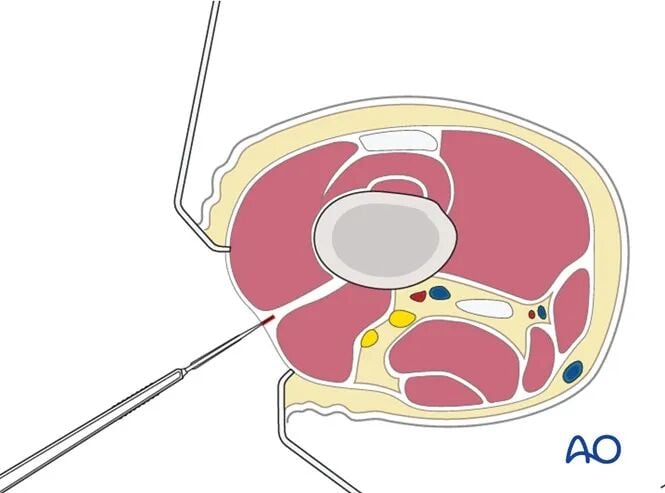
A 1–1.5 cm incision is made in line with the corresponding plate hole.
This incision is made in a single step, cutting through skin, subcutaneous tissue, iliotibial band, vastus lateralis fascia, and the vastus lateralis muscle belly.
Common Mistake:
Making the incision too small. A 1–1.5 cm incision is usually sufficient for most screw insertions.
If two adjacent screws are required, a short version of the lateral approach to the femur can be used for that segment.
Closure
The iliotibial band is closed with absorbable sutures. Subcutaneous tissue and skin are closed in standard fashion.