
Lisfranc Injury Surgical Illustration, AO Standard!
I. Introduction
Compartment Syndrome
More than 25% of Lisfranc injury cases may be complicated by or lead to compartment syndrome. If compartment syndrome is suspected, fasciotomy is required. Swelling will not subside until reduction is achieved. However, soft tissue coverage must still be assessed prior to surgical intervention.
Preoperative Planning
A detailed preoperative plan is strongly recommended for these complex injuries. The planning steps include:
1. Determine which joints are unstable.
2. Determine whether instability is due to bony injury or ligamentous injury.
3. Develop the optimal reconstruction strategy for each injury.
4. Identify the key points for restoring the length of the medial and lateral columns.
5. Assess the need for stabilization of ligamentous injuries and plan accordingly (including intercolumnar ligamentous instability).
General Reconstruction Strategy
Surgical Sequence
Lisfranc injuries are highly heterogeneous and require individualized treatment plans.
A general stepwise reconstruction strategy can be referenced as follows:
1. Restore the normal anatomical relationship between the cuneiforms and the navicular.
2. Restore the normal anatomical relationship between the second metatarsal and the intermediate cuneiform (this serves as the foundation for subsequent reduction).
3. Restore the normal anatomical relationship between the second metatarsal and the medial cuneiform.
4. Address tarsometatarsal joint injuries in the order of 1st → 3rd → 4th → 5th tarsometatarsal joints.
Fixation Principles
- For bony injuries of the 1st–3rd tarsometatarsal joints, reconstruction is the first choice; if reconstruction is not possible, arthrodesis is performed.
- For unstable joints without bony injury, there are no clear guidelines on whether to perform fusion or temporary fixation; the choice depends on surgeon preference and the overall injury pattern. Generally, fusion of the 1st–3rd tarsometatarsal joints has little impact on foot function.
- The 4th–5th tarsometatarsal joints should retain mobility; temporary K-wire fixation is the preferred method.
- Some surgeons prefer to temporarily fix all injuries with K-wires first, verify foot stability and function, and then proceed with definitive plate-and-screw fixation.
Timing of Surgery
The timing of surgery is determined by both the degree of soft tissue injury and the patient's physiological status.

II. Intraoperative Assessment of Joint Instability
Stress views under fluoroscopy can assist with preoperative assessment.
Alternatively, preoperative weight-bearing radiographs (if the patient can tolerate them) may be obtained.
These images help determine ligamentous instability between the cuneiforms and metatarsals.
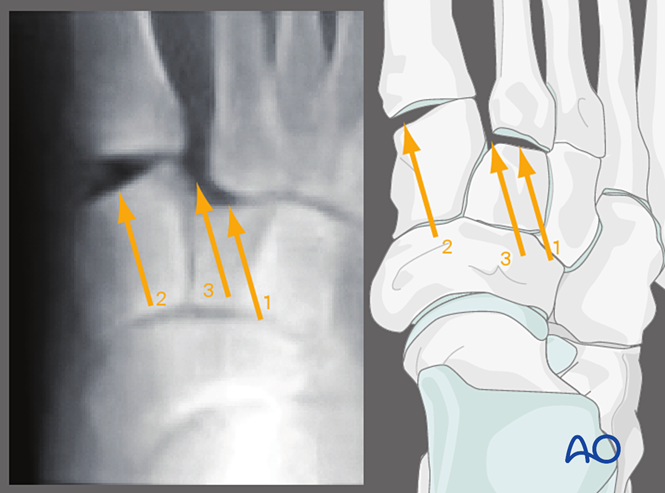
Valgus Stress, AP View
Applying valgus stress allows observation of:
1. Lateral displacement of the second metatarsal relative to the intermediate cuneiform.
2. Disruption of the first tarsometatarsal joint.
3. Widening of the space between the medial cuneiform and the second metatarsal (indicating Lisfranc ligament injury).
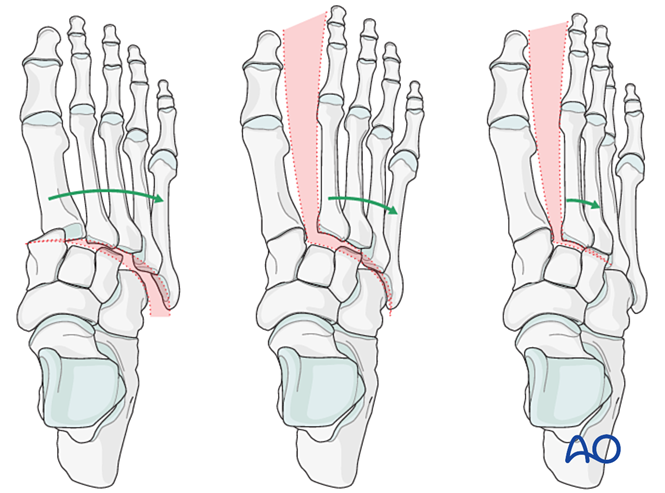
Other findings include:
- Lateral displacement of all metatarsals.
- Lateral displacement of the middle and lateral columns.
- Isolated lateral displacement of the middle column.
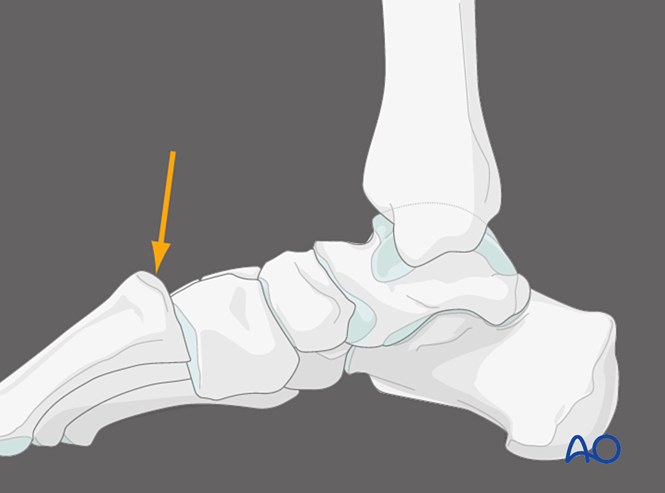
Plantar Pressure on the First Tarsometatarsal Joint, Medial View
Applying pressure on the plantar aspect of the first tarsometatarsal joint can identify dorsal capsular instability. Under normal conditions, the dorsal cortex of the metatarsal should align with the dorsal cortex of the cuneiform. Dorsal displacement of the metatarsal base beyond the plane of the cuneiform indicates instability of the first tarsometatarsal joint.
III. Reduction
Closed Reduction
Under anesthesia, apply axial traction and reverse the mechanism of injury to achieve reduction.
Open Reduction
If closed reduction fails to achieve anatomic reduction of the joint, it may be due to bony block or soft tissue interposition, requiring direct open reduction.
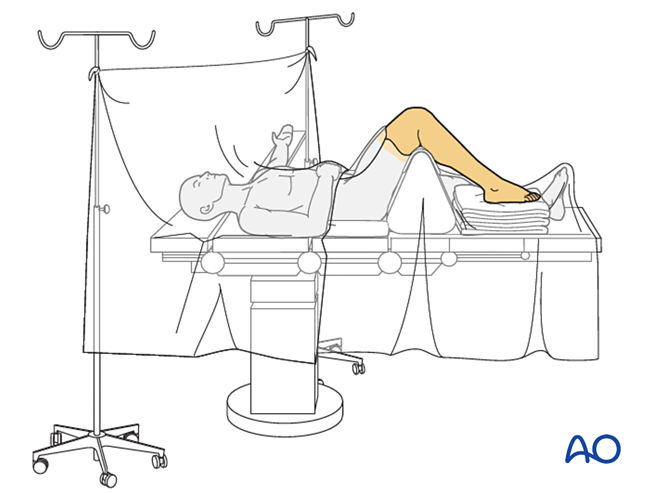
IV. Approach Preparation
The patient is placed in the supine position with the knee flexed to 90°.
Surgical Approach Selection
The choice of approach depends on the fracture pattern. Commonly used approaches include:
- Dorsolateral approach
- Dorsomedial approach
- Medial universal incision
- Percutaneous navicular approach
- Safe zone for K-wire/Steinmann pin placement
- All Lisfranc injuries involve the second tarsometatarsal joint. A slightly extended medial incision can simultaneously address the first and third tarsometatarsal joints.
- Additional stab incisions may be used for placement of lag screws or fiber tape (e.g., for a medial-to-intermediate cuneiform lag screw).
V. Surgical Steps
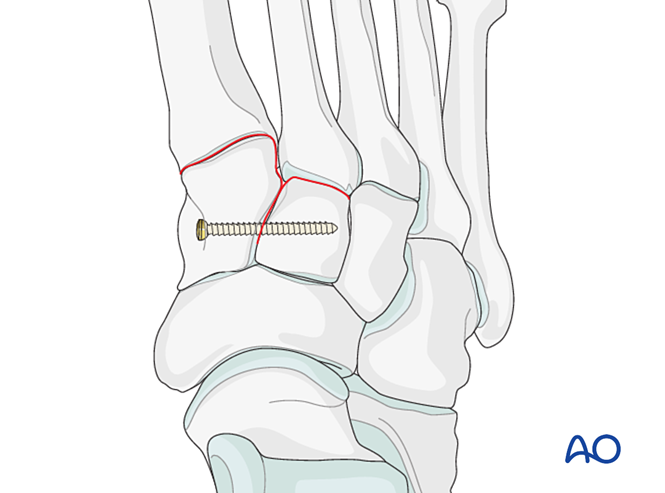
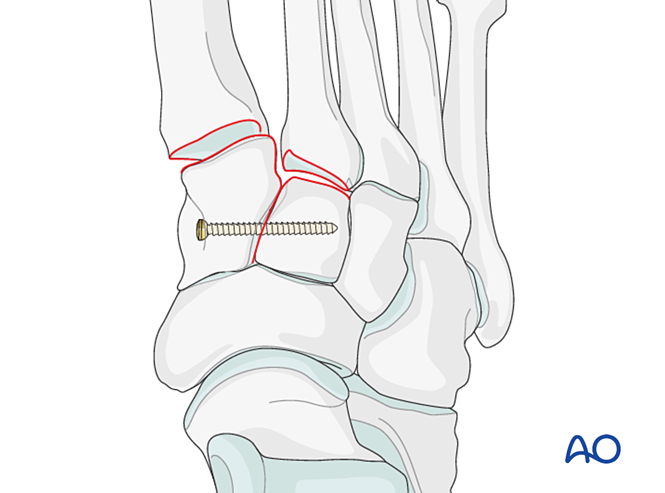
Step 1: Instability Between the Medial and Intermediate Cuneiforms
If injury involves instability between the medial and intermediate cuneiforms, options include temporary/definitive fixation or fusion:
- Place a positioning screw from the medial cuneiform to the intermediate cuneiform (see illustration).
- Elastic dynamic fixation.
- Perform intercuneiform arthrodesis (lag screws must not enter the joint between the medial and intermediate cuneiforms).
Step 2: Second Tarsometatarsal Joint Instability (if present)
Re-establish the anatomic relationship between the second metatarsal and the intermediate cuneiform. This serves as the reference for reduction of the other tarsometatarsal joints; precise alignment is critical.
Ligamentous Instability
Reduction
- Insert a K-wire from distal to proximal intramedullary to serve as a joystick for axial alignment.
- Verify axial alignment on AP view and dorsal/plantar alignment on lateral view under fluoroscopy.
- Advance the K-wire across the joint into the intermediate cuneiform to maintain alignment.
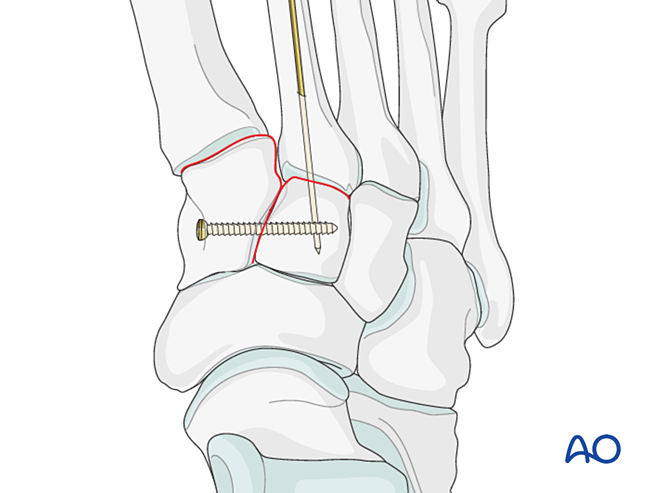
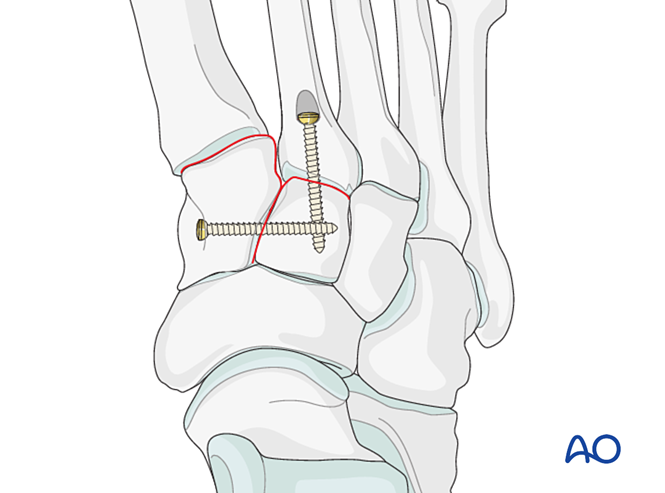
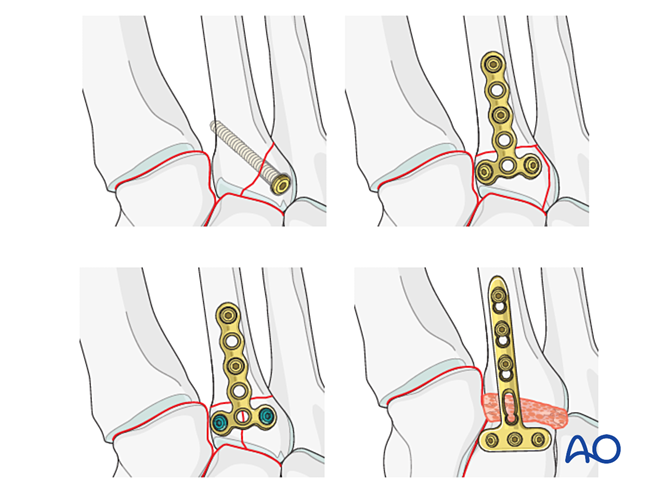
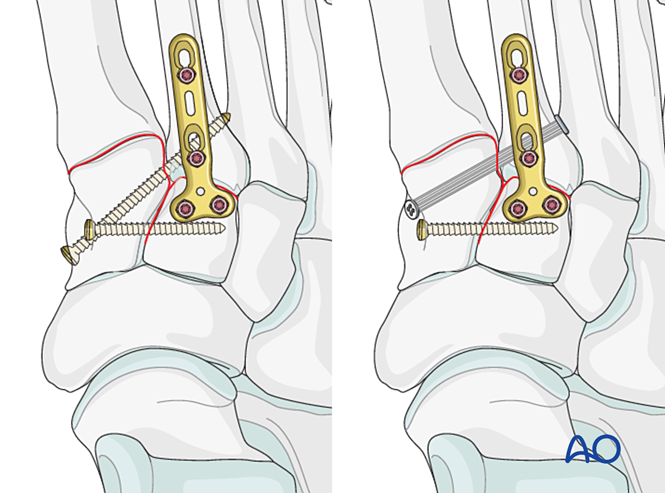
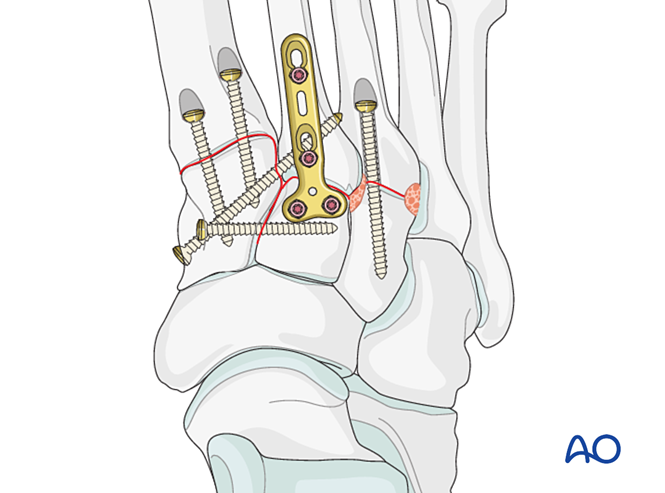
Fixation
- Place a positioning screw across the joint to maintain reduction.
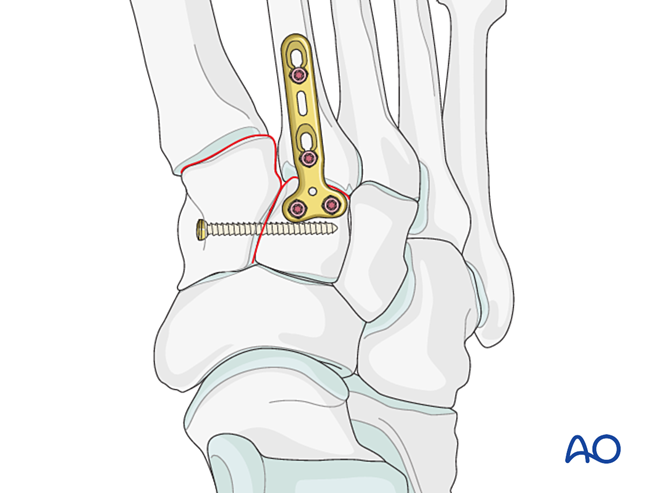
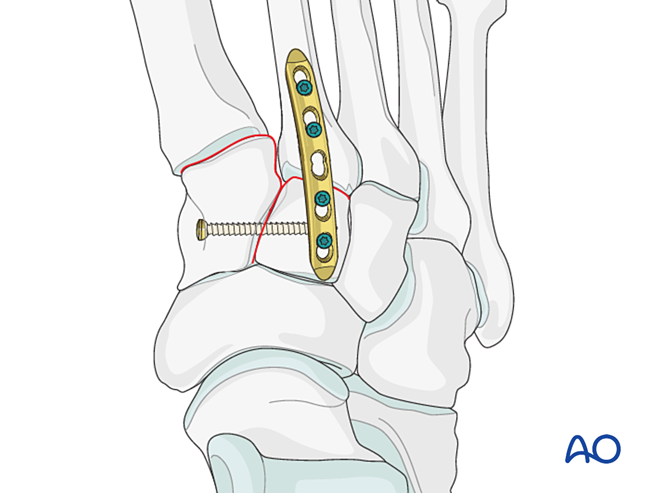
- A mini T‑plate may be used if bone quality permits.
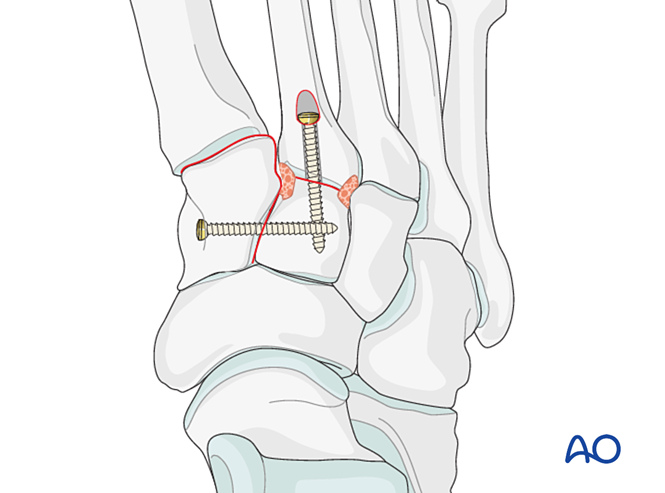
- If arthrodesis is required, prepare the joint, place a transarticular lag screw, and apply bone graft.
- Caution: The lag screw may interfere with other implants (e.g., Lisfranc ligament stabilization device) or be contraindicated due to comminution of the second metatarsal base. In such cases, a Lisfranc plate (or a contoured 2.7 mm locking plate) may be used.
Instability Due to Proximal Second Metatarsal Fracture
Choice of treatment based on fracture type:
- Lag screw (for partial intra‑articular fractures).
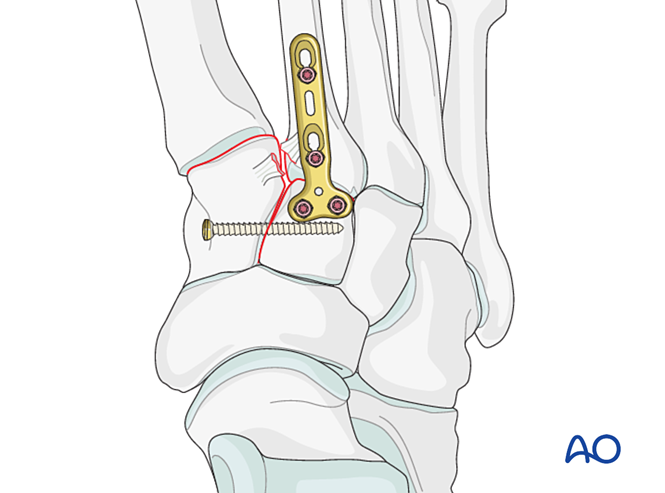
- Plate ± lag screw (for complete intra‑articular fractures where the articular surface can be reconstructed).
- Locking plate ± lag screw (for complete intra‑articular fractures with osteoporosis or where lag screw placement is not possible).
- Primary fusion for length‑stable or length‑unstable fractures (when the articular surface cannot be reconstructed).
If the tarsometatarsal joint remains unstable after reduction and fixation, a bridging plate may be temporarily applied until bone healing occurs. Alternatively, primary fusion can be performed using a transarticular lag screw.
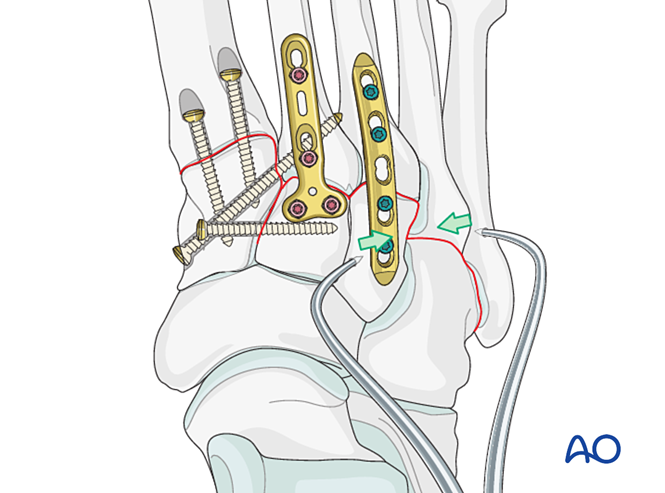
Step 3: Lisfranc Ligament Rupture
Goal: Reduce and compress the second metatarsal base to the medial cuneiform, providing stability.
Lisfranc Instability
Reduction
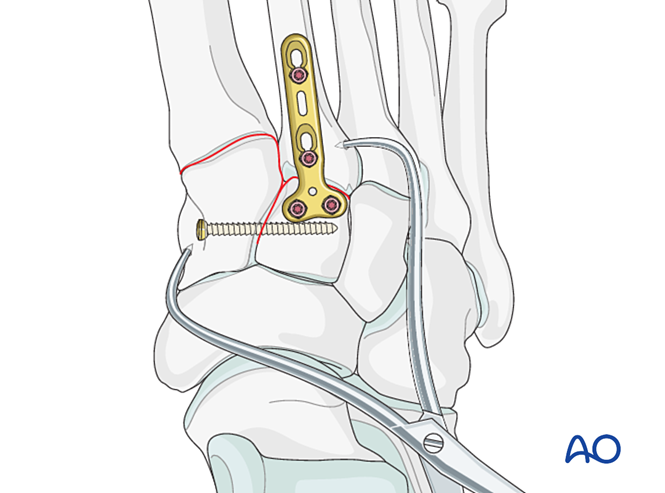
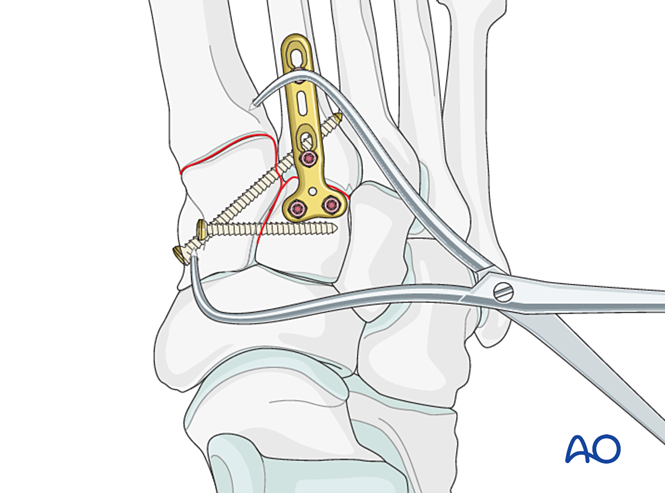
- Pre‑drill holes laterally at the second metatarsal base and medially on the medial cuneiform to facilitate placement of a reduction clamp.
- Use a pointed reduction clamp to reduce the second metatarsal base to the medial cuneiform, taking care to avoid the planned screw trajectory.
- The reduction clamp may be applied percutaneously along the direction of the Lisfranc ligament to provide compression.
- Verify reduction both visually and with fluoroscopy.
Stabilization
Fixation options include:
- Positioning screw from the second metatarsal base to the medial cuneiform (or vice versa).
- Elastic dynamic fixation.
If the second metatarsal base is comminuted, a positioning screw between the first and second metatarsals may be used instead.
Step 4: First Tarsometatarsal Joint Instability (if present)
Ligamentous Instability
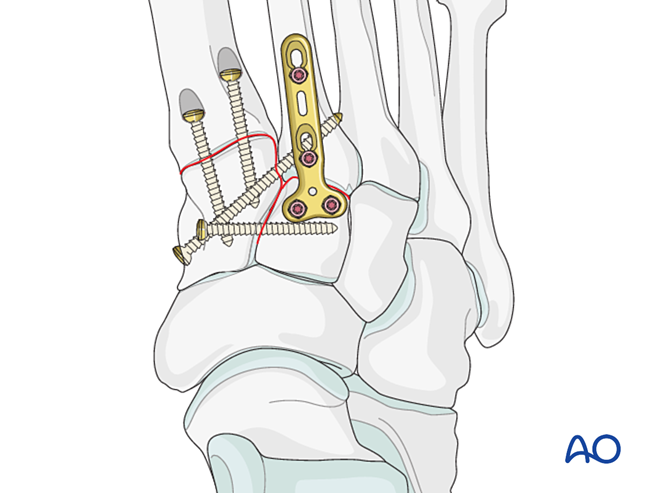
Reduction
For pure ligamentous injury, reduce the joint using a pointed reduction clamp.
Fixation
Place a positioning screw to achieve stability; two screws may be used to enhance stability.
Countersink the screw holes to prevent screw head prominence.
Instability Due to Proximal First Metatarsal Fracture – Treat as described for proximal second metatarsal fractures.
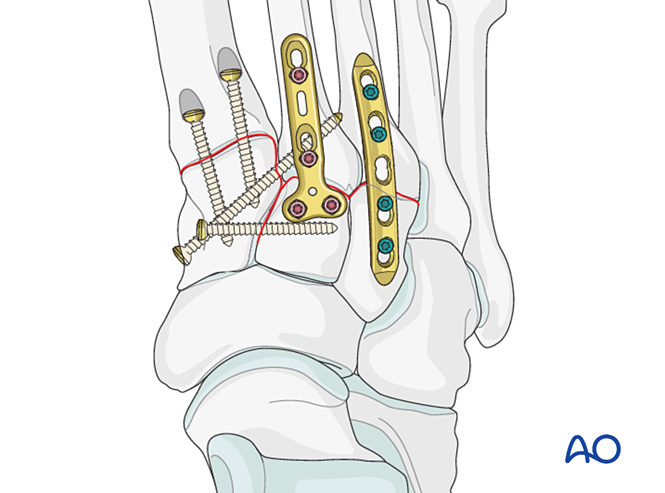
Step 5: Third Tarsometatarsal Joint Instability (if present)
Ligamentous Instability
Reduction
Reduce the joint using a pointed reduction clamp.
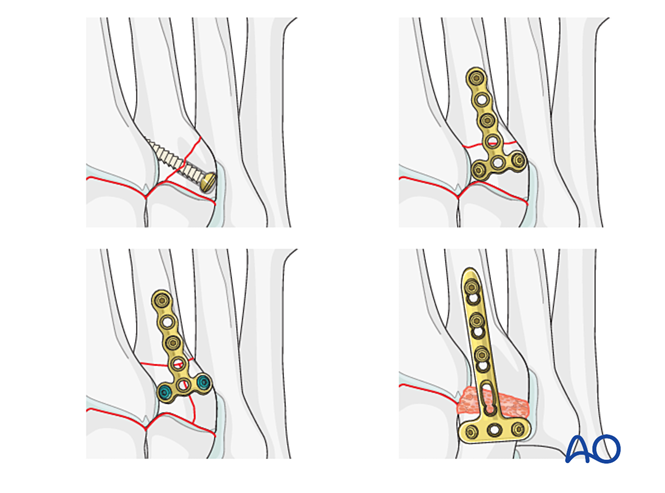
Fixation / Fusion
Place at least one distal‑to‑proximal intramedullary screw to achieve fixation or primary fusion.
Alternatively, a contoured 2.7 mm bridging plate may be used for temporary stabilization until healing. The plate should be contoured to the bone surface and fixed with locking screws or screws in neutralization mode.
Proximal third metatarsal fractures are treated as previously described.
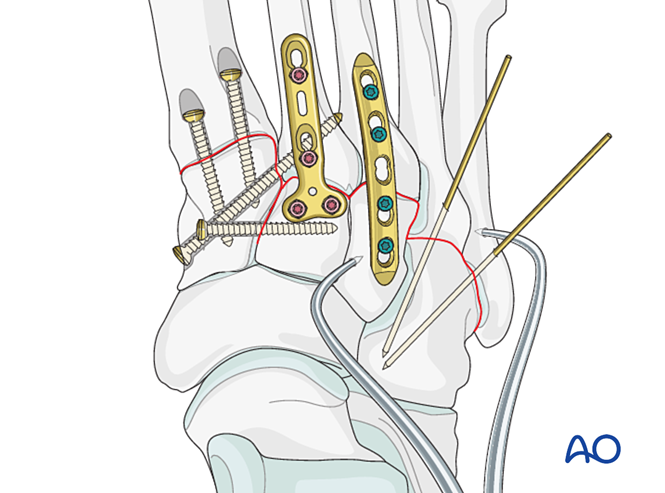
Step 6: Fourth and Fifth Tarsometatarsal Joint Instability (if present)
- Lateral column fractures are first treated according to metatarsal fracture principles, then the fourth and fifth metatarsals are fixed to the cuboid with K‑wires.
- Ligamentous instability or residual instability after medial column fixation is treated as follows.
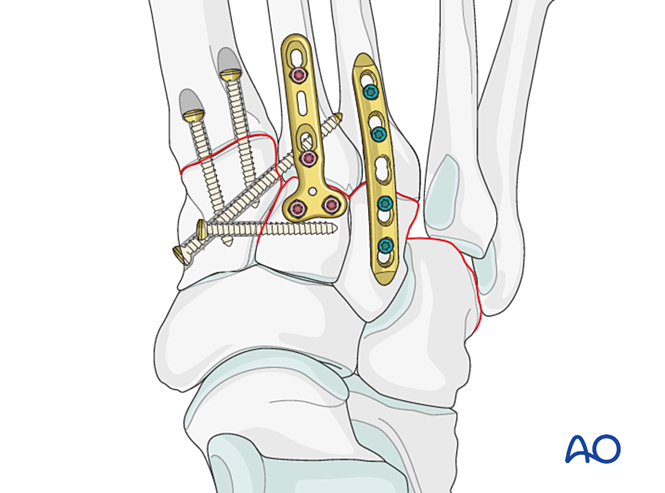
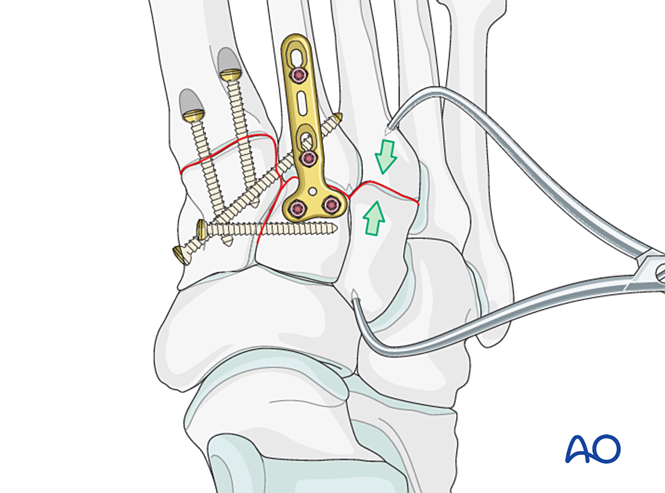
Reduction
Laterally displaced metatarsals must be reduced anatomically to the cuboid using a reduction clamp.
Verify reduction visually and with fluoroscopy.
Fixation
Insert K‑wires from the fourth and fifth metatarsal bases into the cuboid for fixation. Once healed, remove the K‑wires.
VI. Postoperative Care
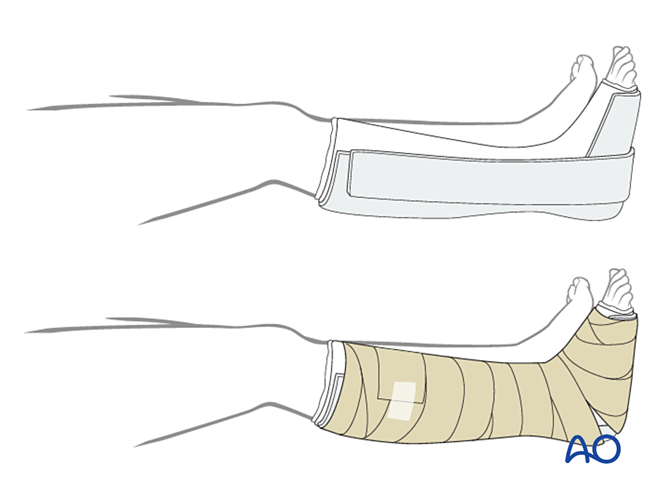
Dressing
The first layer should be a non‑adherent antimicrobial dressing. Wrap the foot from the toes to the knee with sterile padding, reinforcing the medial, lateral, and posterior aspects.
Immobilization
- First two weeks: Use a three‑sided plaster splint, leaving the anterior aspect open to accommodate swelling. Ensure that the vertical parts of the plaster on the medial and lateral sides do not overlap, and avoid pressure on the popliteal fossa and the calf.
- For pure ligamentous injuries treated with elastic dynamic fixation, early weight‑bearing may be allowed, and a walking boot may be used.
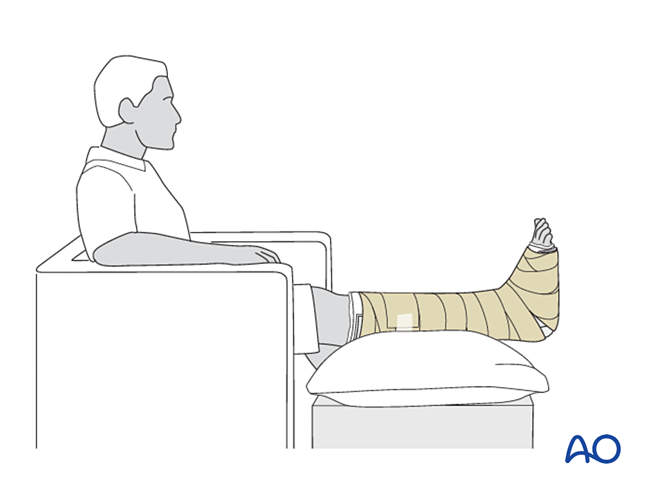
Follow‑up
- Instruct the patient to elevate the injured limb (when seated, the foot should be positioned midway between the waist and the heart). For severe swelling, elevation in the supine position is necessary.
- Avoid direct pressure on the heel to prevent pressure sores.
- The operative dressing is typically left in place until the first postoperative visit at 2 weeks for dressing change and radiographs. If infection or compartment syndrome is suspected, the dressing should be removed earlier for inspection.
- Strict non‑weight‑bearing until radiographic healing is achieved and K‑wires (6–12 weeks) / bridging devices (≥12 weeks) are removed.
- Encourage daily toe movement. Avoid formal physical therapy early on.
- If gastrocnemius contracture develops (more common in midfoot/hindfoot injuries), release may be required.