
Proximal Femoral Fractures: Classification-Guided Treatment
Introduction
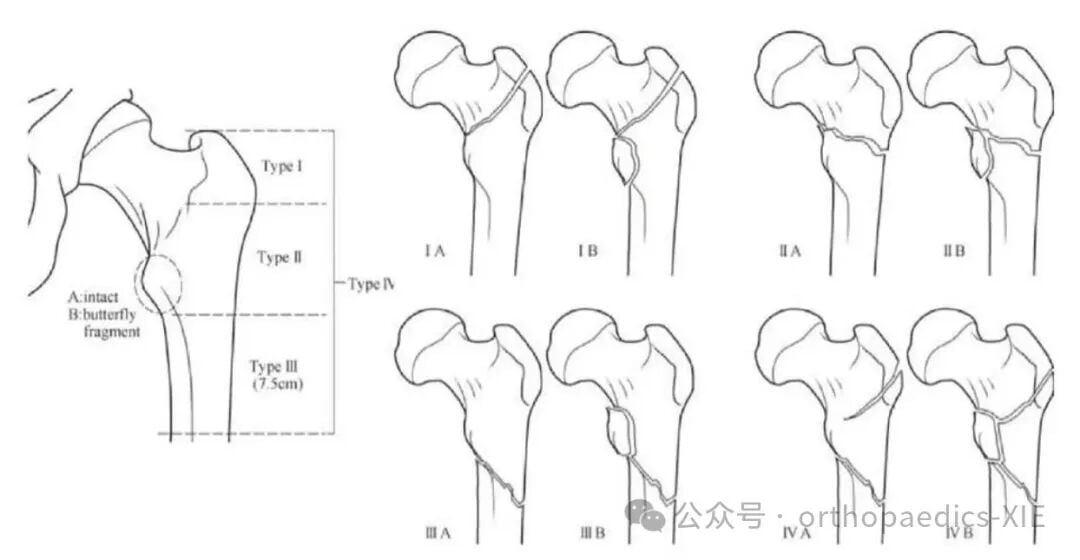
Numerous classification systems (over a dozen) exist for proximal femoral fractures. Most are based on two‑dimensional X‑ray images and focus primarily on medial wall support, while insufficient attention has been paid to the integrity of the lateral wall. Based on the course of the fracture line in the proximal femur, combined with medial wall support and lateral wall integrity, Zhang Zhishan, Zhou Fang and colleagues from Peking University Third Hospital proposed the PUTH (Peking University Third Hospital) regional classification (see figure below).
PUTH Classification
Type I – The lateral fracture line originates between the base of the femoral neck and the lateral apex of the greater trochanter and extends medially to the lesser trochanter, i.e., intertrochanteric fracture.
Type II – The lateral fracture line originates between the lateral apex of the greater trochanter and the lateral cortex corresponding to the level distal to the lesser trochanter; the lateral wall is fractured, i.e., reverse oblique intertrochanteric fracture.
Type III – The lateral fracture line originates between the lateral cortex corresponding to the level distal to the lesser trochanter and the lateral cortex 7.5 cm distal to the lesser trochanter, i.e., subtrochanteric fracture.
Type IV – Complex fractures where the main lateral fracture line is located in the subtrochanteric region, combined with fractures of the lateral wall or greater trochanteric region – i.e., Type III + Type I, Type III + Type II, or Type III + Type I + Type II.
Each type is further divided into subtype A and subtype B based on whether there is a separate fracture fragment in the posteromedial cortex (lesser trochanteric region):
- Subtype A: no separate fragment
- Subtype B: separate fragment present
Treatment Recommendations
The management of intertrochanteric fractures remains controversial. The main factors influencing treatment decisions include:
1. Bone quality
2. Fracture type and complexity
3. Quality of reduction
4. Irreducible fractures
5. Choice of implant
Specific recommendations by fracture type:
Type IA – Dynamic Hip Screw (DHS) or intramedullary fixation is recommended.
Type IB – Intramedullary fixation is recommended.
Type II – Due to an incompetent lateral wall, PFP (locking plate), PFNA, or Intertan is recommended.
Type III and Type IV – Intramedullary fixation is recommended.
Reference
Zeng BF. *OTC Chinese Trauma Orthopaedics Course* (2nd ed). Shanghai: Shanghai Century Publishing (Group) Co., Ltd., Shanghai Scientific and Technical Publishers, 2021:273‑274.