
Gyermekkori supracondylaris humerus-törések kezelése
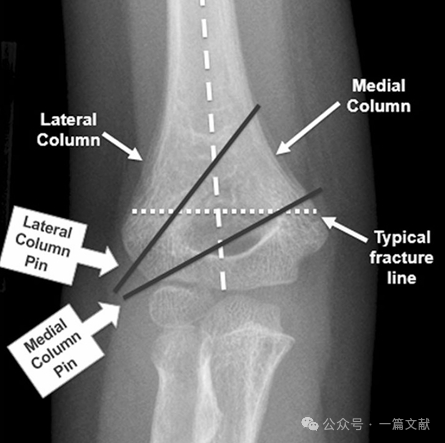
I. A csontok anatómiája: A humerus distalis része egy mediális oszlopból és egy laterális oszlopból áll, amelyeket az ízületi szegmens köt össze. Törés esetén a mediális és a laterális oszlopok elmozdulásra hajlamosak.
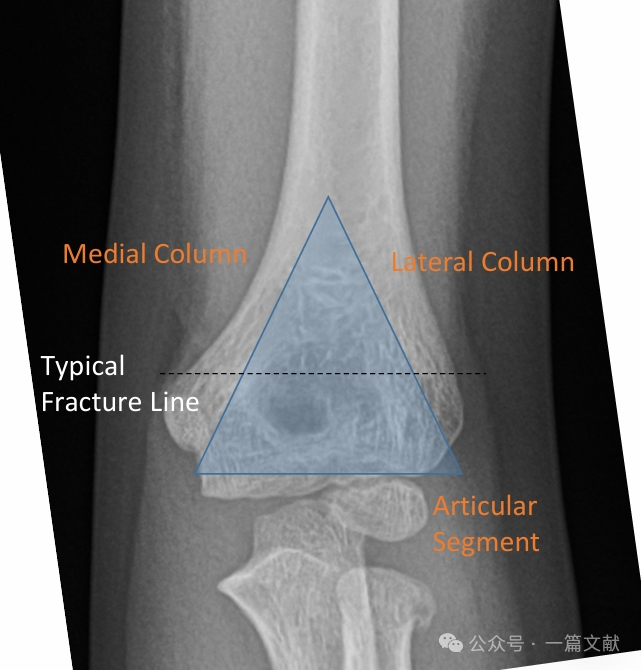
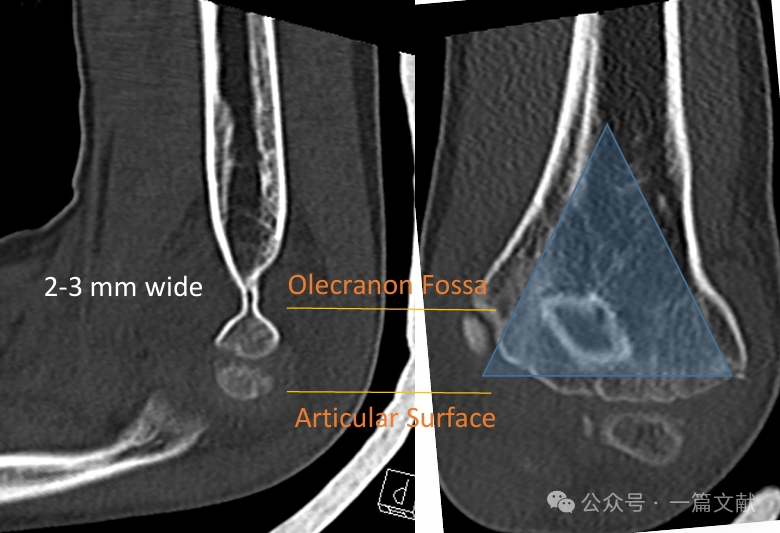
A mediális és a laterális oszlopokat egy vékony csontdarab köti össze az olecranon-fossa területén.
* Ez a terület szerkezeti gyengeségi pontot képez, ezért hajlamos törésre.
* Amikor a könyök semleges helyzetén túl nyúlik (gyerekeknél gyakran hiperextensió), az izmok elvesztik mechanikai előnyüket.
* Az olecranon forgópontként működik.
* Az ízületi tok a kinyújtó erőket a distalis humerusra továbbítja, éppen a physis proximális oldalán.
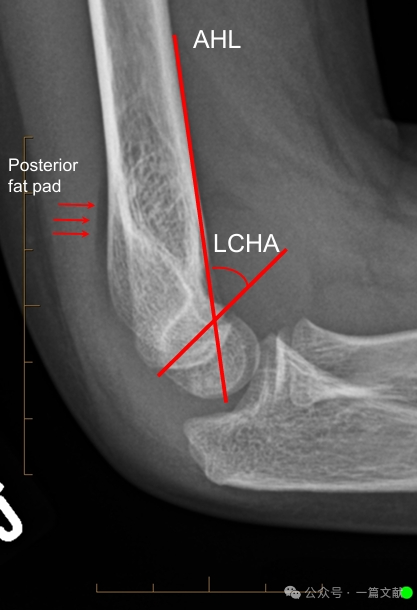
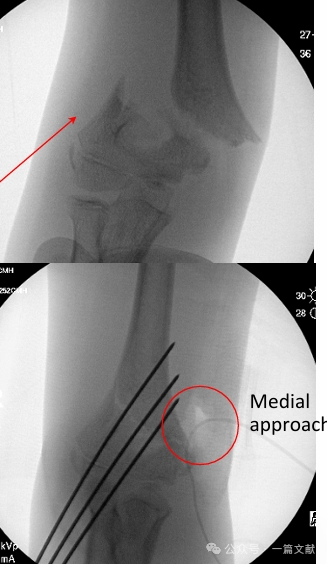
II. Képalkotó vizsgálatok: A röntgenfelvételek általában elegendőek. Könyök AP- és oldalnézeti felvételei szükségesek. Az azonos oldali alkar/csukló röntgenfelvételeit is el kell készíteni a kapcsolódó sérülések értékelése érdekében. A nem elmozdult törések esetében értékelni kell a hátsó zsírpárna-jelenséget (a nyíllal jelölt terület).

Oldalnézeti röntgenfelvételen való egyenesítés:
* Elülső humerális vonal (AHL): Át kell haladnia a capitellum osszifikációs középpontján.
* Capitelláris elülső szög: 30–40 fok.
* Oldalsó capitellohumerális szög (LCHA): Kevesebbnek kell lennie, mint 69 fok.
* Hátsó zsírpárna jel: Erősen sugallja a törést (míg az elülső zsírpárna jel akkor is megjelenhet, ha nincs törés).
Igazítás AP röntgenfelvételen:
* Baumann-szög: A humerus tengelyére merőleges vonal és a capitellum epifizáris rétegén átmenő vonal által bezárt szög. Ennek a szögnek széles a normál tartománya (9–26 fok). A normális érték meghatározásának legjobb módja a contralaterális összehasonlító felvétel készítése.

III. Töréstípusok: Gyakori extenziós és flexiós típusú sérülések.
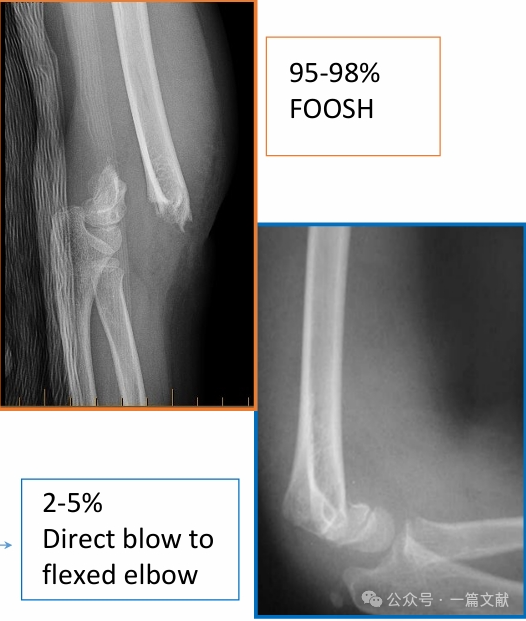
Extenziós típusú sérülések:
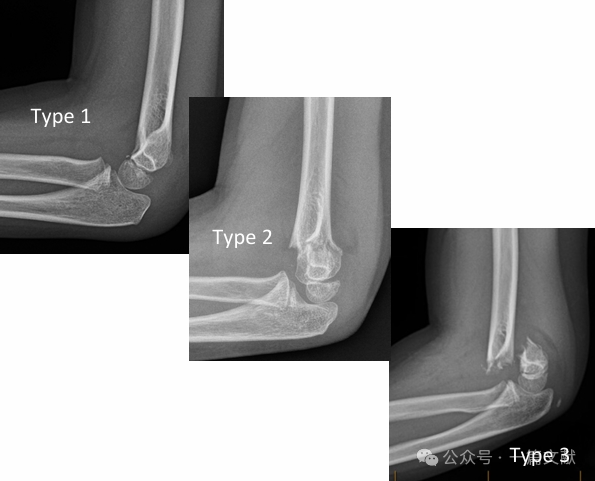
* Klasszikus Gartland-osztályozás:
* 1. típus: Elmozdulatlan.
* 2. típus: Elmozdult törés, de érintetlen hátsó csuklóhurkokkal.
* 3. típus: Elmozdult törés a hátsó csuklóhurkok megszakadásával.
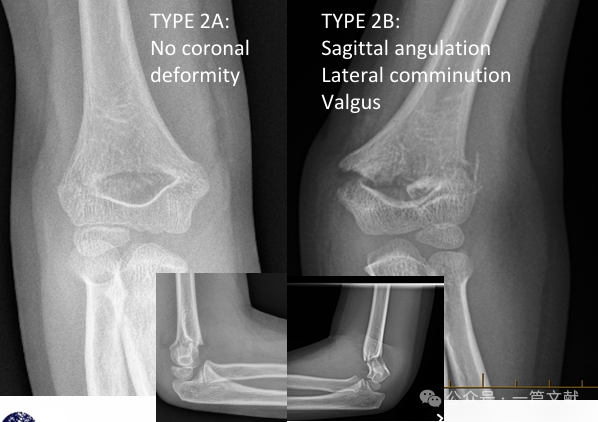
* Módosított Gartland-osztályozás:
* 2A típus: Csak a szagittális síkban fellépő szögeltérés. Zárt redukció és hosszú karra kiterjedő gipszbe kötés alkalmazható, de szoros követés szükséges.
* 2B Típus: Forgó, koronális síkbeli szögeltérésű (varus, valgus) és/vagy eltolódásos komponensű törés. Társulhat töredékes törés vagy beszorulás is. A zárt redukció egyedül (percután szegélyezés nélkül) magas sikerrátája van. A zárt redukció és percután szegélyezés (CRPP) ajánlott.
* Típus 3: Teljes hátsó elmozdulás a hátsó csuklóhurkok mechanizmusának megszakadásával; a periosteális hüvely érintetlen.
* 4. típus: Instabil mind a flexió, mind az extenzió során; a periosteális hüvely megszakadt.
* A 3. típus és a 4. típus megkülönböztetése: A megkülönböztetést intraoperatívan, fluoroszkópiával végezzük, amikor a beteg érzéstelenítés alatt áll – ez egy intraoperatív megkülönböztetés.

Hajlításos típusú sérülések:
* Jellemző rájuk a nagyobb általános instabilitás és a magasabb szövődmény-gyakoriság. Társulhat ulnáris ideg tünetekkel.
* Kezelés: Bármely elmozdulás esetén zárt redukció és perkután clippelés (CRPP) szükséges. Ezek a törések gyakrabban igénylik a nyitott redukciót és perkután clippelést, mint a hajlításos típusú törések.

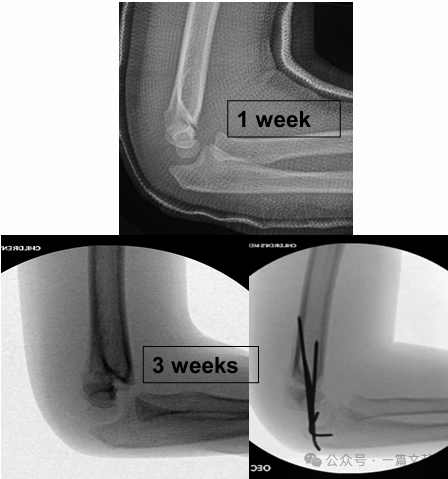
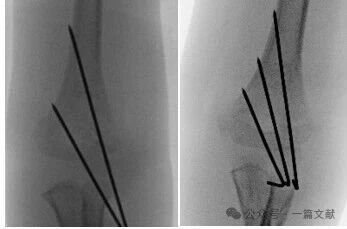
IV. Konzervatív kezelés: Kerülni kell a duzzadt könyök beöntését 90 foknál nagyobb flexióban. A szoros követés különösen fontos, főként a 2-es típusú töréseknél. Ha csak zárt redukcióval kezelik, az első hét során a redukció elvesztésének aránya akár 48%-os is lehet. A diszlokáció kockázati tényezői: nagyobb kezdeti elmozdulás, 2B típusú törések és nagyobb felső kar kerületű betegek. Ahogy a képen látható, egy konzervatív kezelésben részesült betegnél a 3. héten végzett követő röntgenfelvételen töréselmozdulást észleltek, majd később K-drótos sebészi rögzítést végeztek.
V. Sebészi kezelés:
Zárt redukciós technika:
* Hosszanti húzás alkalmazása a hosszúság helyreállításához (kombinálható „tejelési” manőverrel).
* A koronális síkbeli eltolódás korrekciója.
* A szagittális síkbeli eltolódás korrekciója az olecranonra gyakorolt nyomással, amellyel a distalis töredéket anterior irányba tolják el és a könyököt hiperflexióba hozzák.
* Alkar helyzete: pronáció vagy szupináció.

„Bütyök szabálya": A hüvelykujjat a távoli töredék kezdeti elmozdulásának irányába kell mutatni.
* Hátsó-belso elmozdulás → A pronáció meghúzza a belső lágyrész-csuklót.
* Hátsó-külső elmozdulás → A szupináció meghúzza a külső lágyrész-csuklót. (Az ábrán látható)

Elfogadható redukciós kritériumok:
* Az anterior humerális vonal áthalad a kapitellumon.
* Nincs jelentős rés (ez lágyrész-behajlást jelez).
* Nincs varus (Baumann-szög növekedett).
Nyitott redukciós technika:
* Metszetválasztás elve: Kövesse a metafizáris tarajt.
* Előoldali megközelítés: A hátsó elmozdulás, illetve az ér- és/vagy középső ideg sérülés esetén javasolt.
* Belso oldali megközelítés: A hátsó-oldalsó elmozdulás vagy hajlítási típusú sérülések esetén javasolt.
* Oldalsó megközelítés: A hátsó-belső elmozdulás esetén javasolt.
* Hátsó megközelítés: Általában kerülni kell; rosszabb eredményekhez (merevség, érvérontásos nekrózis, esztétikai aggályok) társul.
* Kerülje a sérült szöveti síkokat.
* A további lágyrészek károsodásának minimalizálása.
* Az ábra szerint: posterolaterális elmozdulással járó törés esetén nyitott redukcióra medialis megközelítést alkalmaztunk.
K-drót rögzítési technikák:
* Csak laterális rögzítés:
* A leggyakrabban alkalmazott technika.
* Két vagy három laterálisan elhelyezett K-drótot is lehet használni.
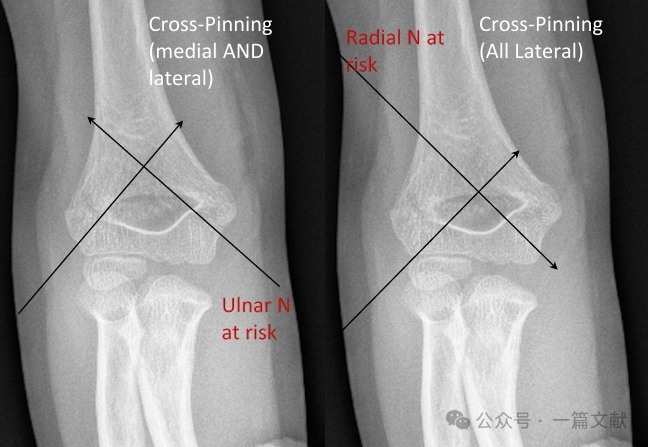
* Keresztrögzítés (medialis és laterális):
* Biomechanikai stabilitást biztosít.
* Iatrogén ulnáris idegsérülés kockázatát hordozza.
* Teljesen laterális rögzítés (divergens):
* Kockázatot jelent a sugárszervi ideg sérülésére.
* Kevesebb gyakorisággal használják.
* Előrefelé irányuló csontvelőbeli clavizáció: Szintén leírták. Megfelelő a magas szuprakondiláris törések kezelésére.
* Biomechanika: A keresztpin-technika biomechanikailag a legstabilabb konstrukció. Azonban a legtöbb 3. típusú törés esetében a keresztpin-technika nem mutatott egyértelmű klinikai előnyt a csupán laterális pin-technikához képest. A keresztpin-technika nagyobb kockázatot jelent az iatrogén ulnáris idegsérülésre (4,3-szorosan növekedett kockázat).
* A mediális pin-technika indikációi:
* Mediális comminutio.
* Proximális mediális–distalis laterális ferde törési minta (fordított ferde törés).
* Intraartikuláris variáns törések. (Lásd az ábrán.)

* Mediális tűzési technika:
* Először helyezzen el két laterális K-tűt.
* Hajtsa a könyököt 45 fokra, hogy lazítsa az ulnáris ideget.
* Figyeljen az ulnáris ideg szubluxációjára (kb. 16% gyermeknél fordul elő, Zaltz 1996).
* Az ulnáris ideg védelme érdekében használjon hüvelykujjas retrakciót vagy kis metszetet a tűk bevezetése során.
* Műtét utáni iatrogén idegbénulás: Vita folyik arról, hogy a tűket el kell-e távolítani.
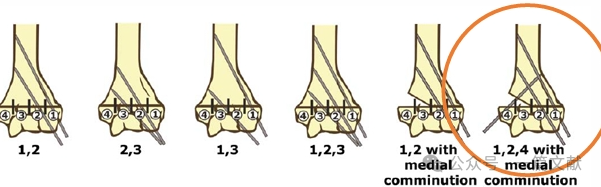
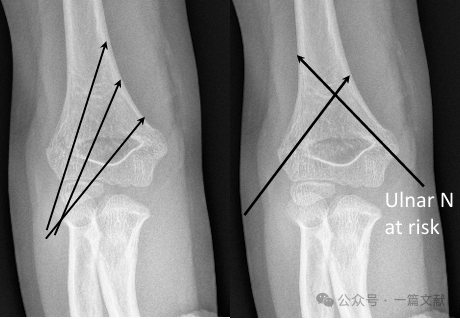
* Ideális tűhelyezési követelmények: 1,5–2 mm-es K-tűket használjon. A tűknek a mediális és laterális oszlopokba kell beérniük divergens mintázatban. A tűk közötti nagyobb távolság növeli a stabilitást. Az ábrán látható a 2A, 2B és 3 típusú törésekhez ajánlott tűelrendezés.

* Érje el a töréshelyen a széles szétválasztást.
* A tűknek a metafízis kiszélesedését követniük kell, hogy rögzítsék a laterális oszlopot.
* A laterálisan elhelyezett tűk segítségével rögzíthető a mediális oszlop.
* A tűhegyeknek a törésvonal közvetlen proximális oldalán kell bekapcsolódniuk a distalis töredékbe.
* További stabilitás érdekében egy harmadik tűt is be lehet vezetni a két fő tű közé.
Műtét közbeni fluoroszkópos stabilitásvizsgálat:
* Ellenőrizze az AP-irányú egyenesítést a könyök kinyújtott helyzetében.
* Készítsen igazi laterális felvételt az egyenesítés értékeléséhez.
* Készítsen ferde felvételeket a mediális és a laterális oszlop redukciójának értékeléséhez.
* Fontolja meg a dinamikus fluoroszkópos stresszfelvételek készítését a redukciós konstrukció stabilitásának értékelésére (különösen akkor, ha korlátozott a követési időszak).
* Elől- és hátulnézet (AP-nézet): Alkalmazzon rotációs, varus/valgus stresszt.
* Oldalnézet: A hajlítás és a nyújtás tartományának értékelése.

VI. Műtét utáni kezelés:
A műtét utáni duzzanatból eredő szövődmények megelőzése érdekében használható gipsz kivágással (az ábrán látható módon).

A K-drótokat általában a műtét után 3–4 héttel távolítják el.
VII. Összefoglalás:
* A műtét előtti gondos ideg-érrendszeri vizsgálat döntő fontosságú.
* Ne hagyjuk ki az azonos oldali társult töréseket („lebegő könyök” sérülések).
* A 2A típusú töréseket zárt redukció és gipszbe helyezés útján lehet kezelni.
* Egyes nem műtéti kezelés alá eső eseteknél szoros követés szükséges.
* A műtét időzítése csak akkor sürgős, ha érrendszeri kompromittálódás jelei mutatkoznak.
* A sebészi kezelés általában zárt redukciót és percután clippelést (CRPP) és annak módosításait foglalja magában.
* A gyermekkori supracondylaris humerus-törések kezelésében eltérő módszerek léteznek.