
التصحيح المفتوح والتثبيت الداخلي باستخدام لوحة تثبيت للكسر الهوفي
أولاً: المبادئ
الاعتبارات العامة
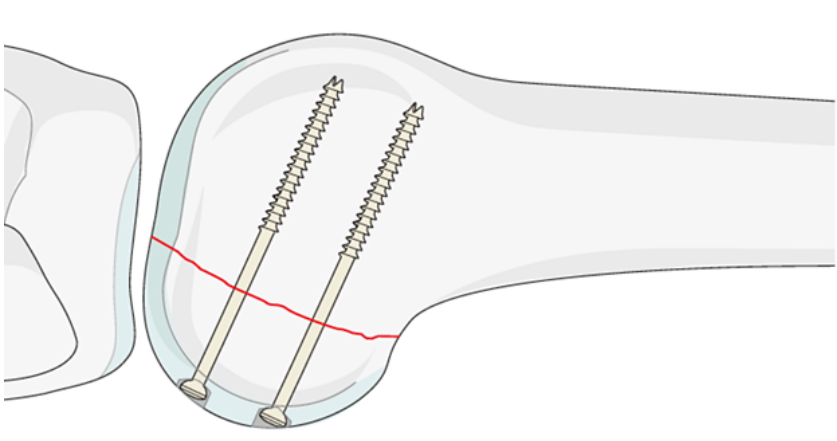
تكسرات هوفا تؤثر في مناطق تحمل الوزن الحرجة داخل مفصل الركبة، وتحتاج إلى تصحيح تشريحي وتثبيت مستقر تمامًا. وعمومًا، يُوصى باستخدام لوحة داعمة جنبًا إلى جنب مع براغي التثبيت المُحكمة. ومع ذلك، إذا كان الجزء المكسور صغير الحجم، فقد تكون البراغي المُحكمة وحدها هي الطريقة الوحيدة الممكنة للتثبيت. ولا يُوصى باستخدام تقنية البراغي المُحكمة غير المباشرة من الوجه الأمامي، لأن الخيوط الطويلة جدًّا لا توفر استقرارًا كافيًا أو ضغطًا فعّالًا على الأجزاء المكسورة. وإذا أصاب الكسر كلًّا من الظرفين (اللذين يشكلان سطح المفصل)، فإن المبادئ نفسها تنطبق.
أنواع البراغي
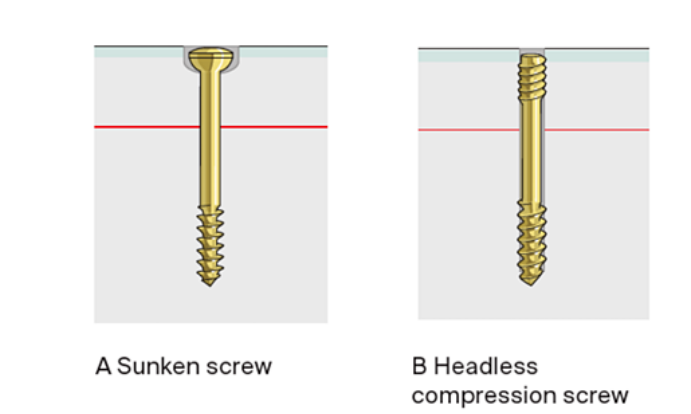
يجب ألا تبرز جميع الغرسات فوق السطح المفصلي. ويمكن تحقيق ذلك باستخدام مسامير لاقطة غاطسة (أ) أو مسامير ضاغطة بلا رأس (ب). ولمنع دوران القطعة، يجب استخدام ما لا يقل عن مسمارين. وفي هذه العملية، يمكن اختيار مسامير ضاغطة بلغة 3.5 مم ذات تجويف أو مسامير لاقطة قياسية بقطر 3.5 مم. ومع ذلك، قد تُستخدم أحجام أخرى من المسامير حسب أبعاد القطعة.
ثانياً: وضعية المريض والمنفذ الجراحي
وضع المريض
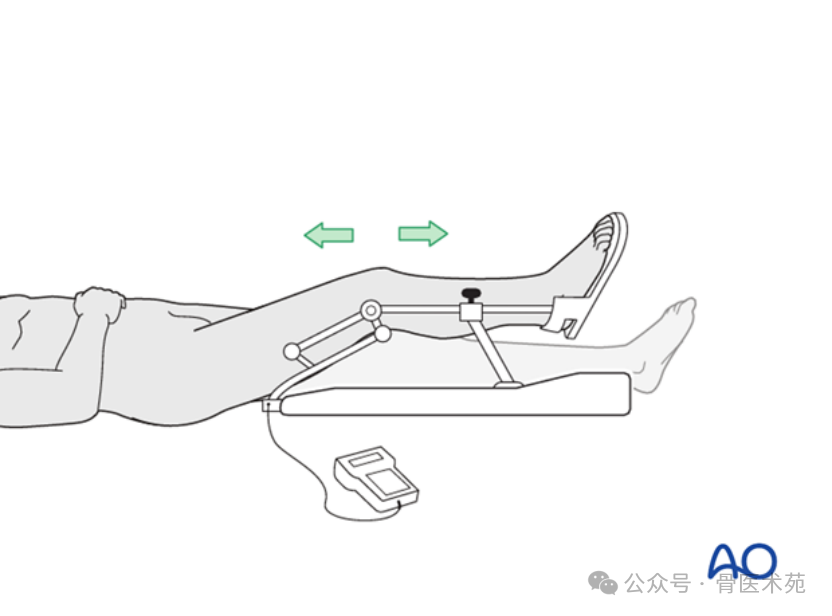
يوضع المريض في الوضع المستلقي على الظهر مع ثني الركبة بزاوية تتراوح بين ٢٠° و٣٠°.
نهج جراحي
- بالنسبة لكسر هوفا الجانبي، يمكن استخدام المنفذ الجراحي «سوشباكلي» أو منفذ استئصال العُرقوب الجردي.
- وبالنسبة لكسر هوفا الإنسي، يُستخدم المنفذ الجراحي الإنسي بين الأعصاب.
ثالثاً: التثبيت
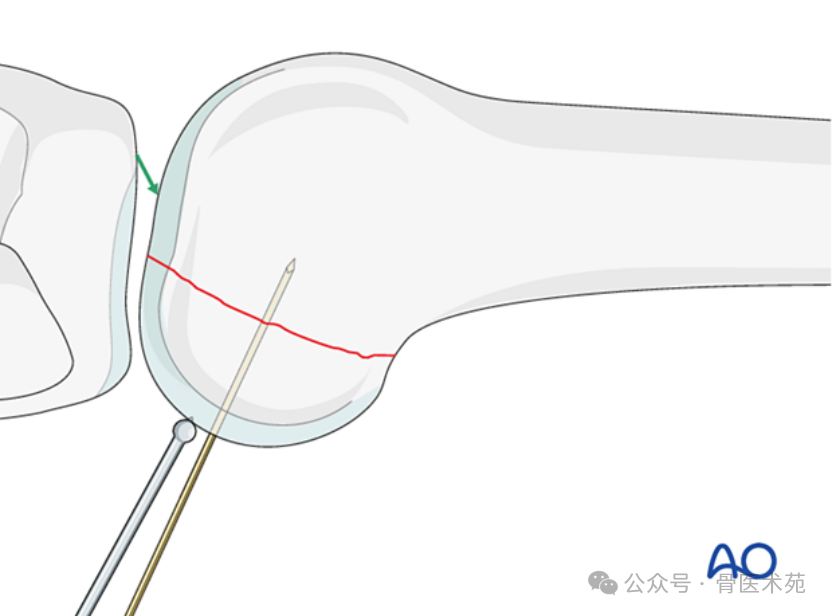
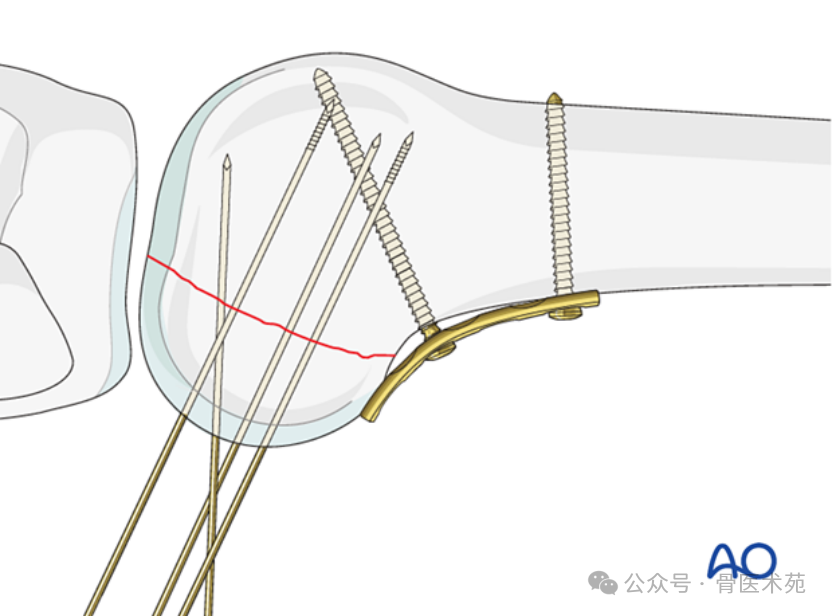
استخدم ملقاط خفض ذي طرف كروي صغير أو مسمار عظمي لتثبيت الكسر، ثم ثبّته مؤقتاً بواسطة أسلاك كيرشنر. وتأكد من أن مواضع أسلاك كيرشنر لا تتعارض مع مكان لوحة التثبيت المخطط لها ومسارات المسامير.
رابعاً: التثبيت
مبدئياتها
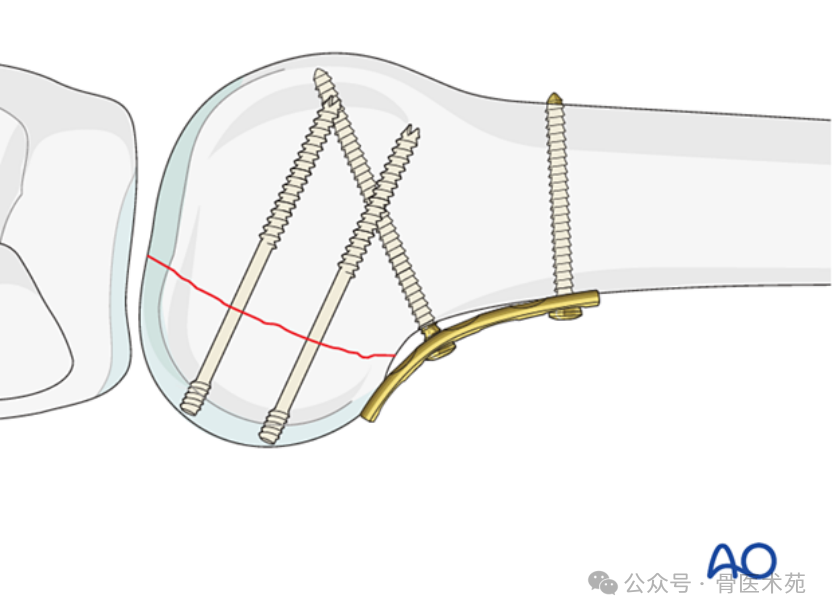
لتحسين الاستقرار وتجنب التحميل المحوري في موقع الكسر (وخاصة في العظم الهش)، تُستخدم لوحة داعمة لمنع التحول الطرفي للقطعة. وتُوضع اللوحة وفقًا لموقع القطعة غير المستقرة؛ وأحيانًا تقع هذه القطع في الجانب الوحشي. وتتوفر أنواع مختلفة من الألواح؛ فعلى سبيل المثال، يستخدم هذا النص لوحة ضيقة بسمك ٣,٥ مم منخفضة الارتفاع لتوضيح الفكرة.
تطبيق اللوحة
تُطبَّق اللوحة على السطح الخلفي للطرف البعيد لعظمة الفخذ. ويجب وضعها في أقصى موقع طرفي ممكن مع تجنُّب سطح المفصل. وللسماح للوحة منخفضة الارتفاع بأن تتبع شكل عظمة الفخذ بدقة، يُدخَل برغي قشري قياسي في الوضع المحايد بالقرب من الجزء القريب من خط الكسر.
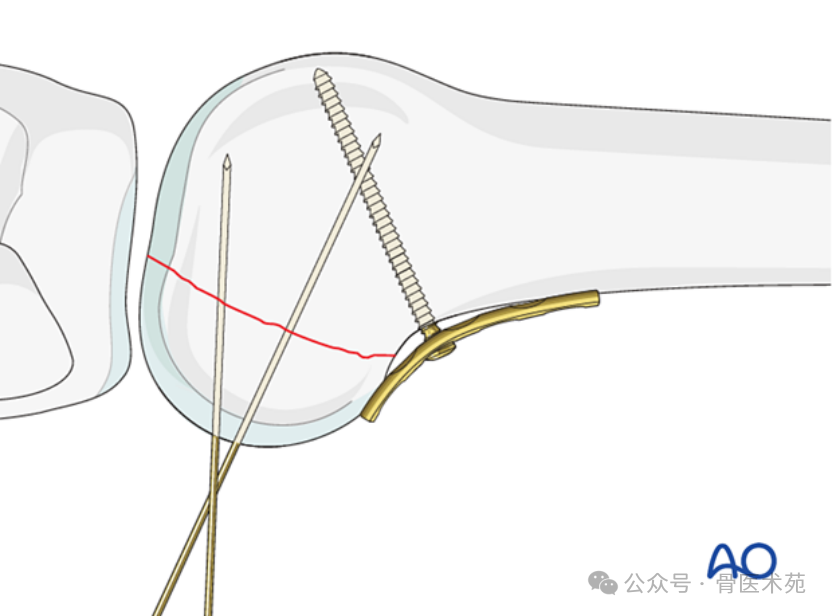
إدخال البرغي في الوضع المحايد
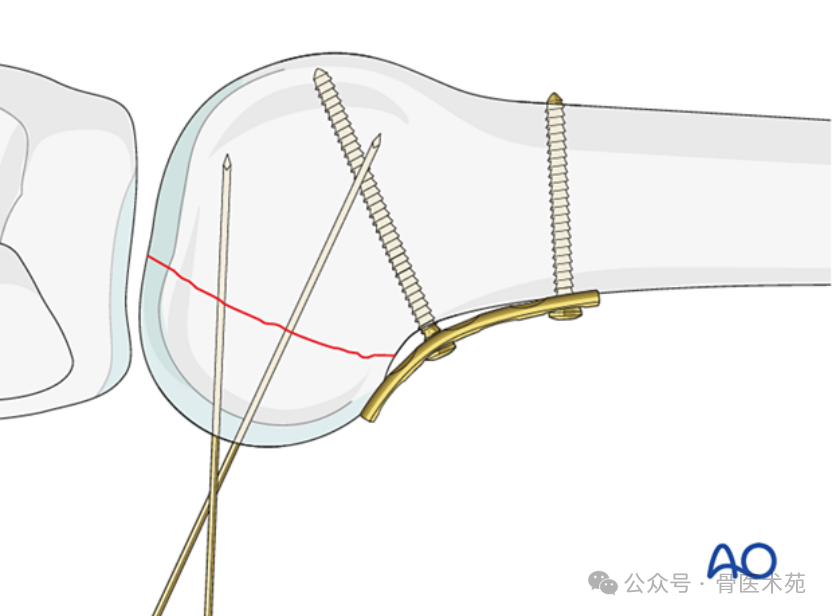
ثبّت اللوحة في الاتجاه القُرباني باستخدام برغي أو أكثر ثنائي القشرة موضوعة في الاتجاه القُرباني بالنسبة للبرغي الأول. وإذا أمكن إدخال البراغي في المناطق غير المفصلية، فيجوز إدخال براغي إضافية في الاتجاه البعدي للوحة. ويُدخل جميع البراغي في الوضع المحايد.
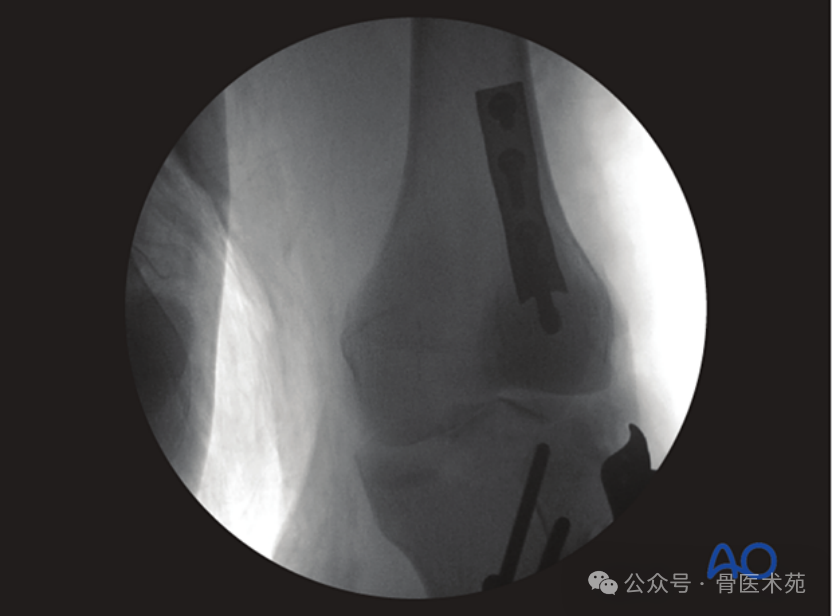
صورة أثناء الجراحة
تظهر الصورة المُلتَقَطة أثناء الجراحة كسر هوفا الخلفي بعد تثبيته مؤقتًا بواسطة أسلاك كيرشнер (K-wires)، مع تعزيزه بلوحة داعمة خلفية.
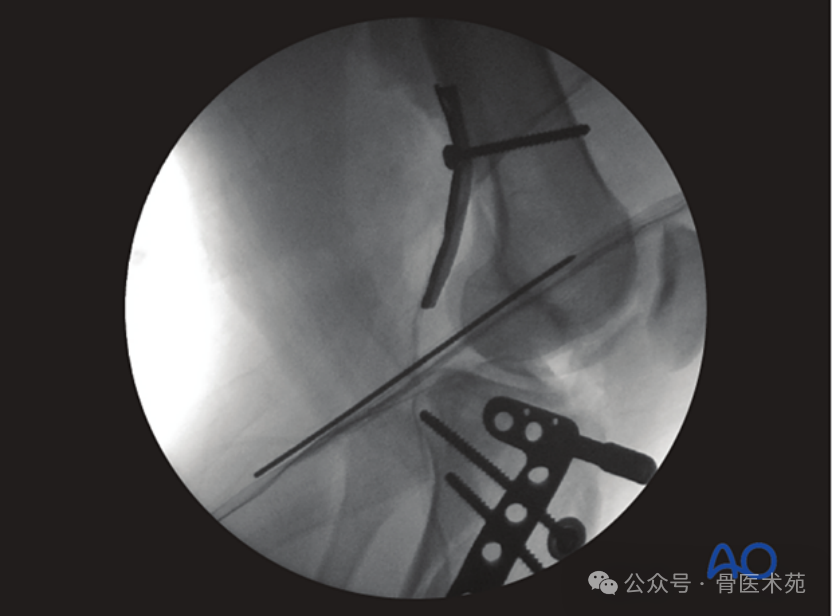
صورة شعاعية بعد الجراحة
تؤكد التصويرات بعد الجراحة وضع اللوحة الداعمة الخلفية بشكلٍ صحيح.
وضع السلك الإرشادي
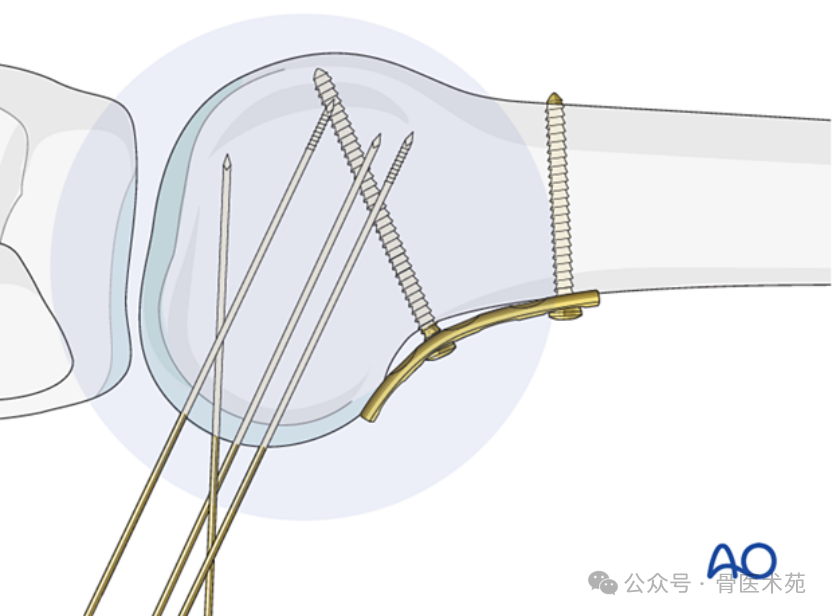
أدخل سلكين إرشاديين عموديَّين على مستوى الكسر، مع التأكّد من أنّهما لا يخترقان القشرة البعيدة.
التحقق من موقع السلك الإرشادي
تحقّق من موقع السلكين الإرشاديين تحت التحكم بالمشعّاع الضوئي (Image Intensifier) من المنظور الجانبي والمنظور المائل.
إدخال البراغي الانضغاطية بدون رأس
استخدم مفك براغي مجوفًا لإدخال براغي الضغط بدون رأس، وتحقق من طول البرغي المناسب تحت رؤية التصوير المُكثَّف الجانبي.
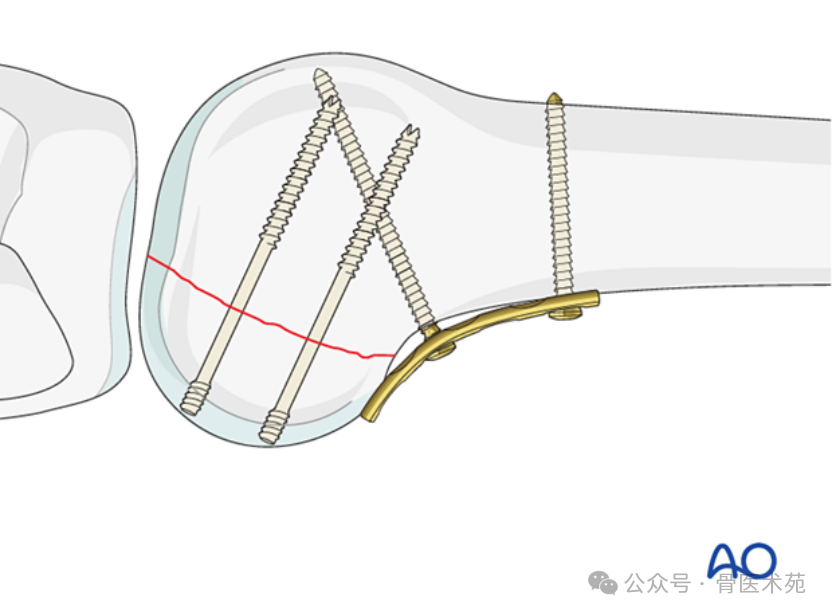
إدخال برغي التثبيت الإسفنجي
بديل: استخدام البراغي القياسية – أدخل براغي التثبيت وفقًا للتقنية القياسية المستخدمة في براغي التثبيت الإسفنجي، مع التحكم بالتصوير المُكثَّف. اغمر رؤوس البراغي لتفادي بروزها.
خامسًا: مثال سريري
كما هو موضح في الشكل، إذا وُضِع اللوح جانبيًّا أو وسطيًّا بدلًا من الوضع الخلفي، فإن فشل التثبيت يكون محتملًا للغاية. ويظهر الصورة عدم تناسق في السطح المفصلي، ما يستدعي إجراء جراحة تصحيحية.

سادسًا: إعادة التأهيل بعد الجراحة
بعد كسور الفخذ البعيدة، تشمل العوائق الرئيسية أمام استعادة وظيفة الركبة بالكامل التليّف والالتصاقات في الأنسجة الرخوة المحيطة بمنطقة الكسر الانتهائي، والتندّب الغشائي، والالتصاقات داخل المفصل، وضعف العضلات. وتساعد تمارين الحركة المبكرة في استعادة حركة المفصل في المرحلة المبكرة بعد الجراحة. وبشرط أن يكون تثبيت الكسر مستقرًّا، يضع الجرّاح وأخصائي العلاج الطبيعي خطة إعادة تأهيل تدريجية مُصمَّمة خصيصًا لكل مريض. والتعليمات المقدمة هنا هي لأغراض الإرشاد فقط، وليست إلزامية.
العلاج الوظيفي
ما لم تكن هناك إصابات أو مضاعفات أخرى، يمكن البدء فورًا في حركة الركبة بعد الجراحة. ويمكن البدء بالحركات النشطة والسلبية للركبة والورك في اليوم الأول بعد العملية الجراحية. وينبغي أن يركّز العلاج على التقوية التدريجية لعضلة الفخذ الأمامية (الرباعية الرأس) ورفع الساق المستقيمة.
التحمل الوزني
يمكن البدء فورًا بعد الجراحة في التحمّل الوزني الخفيف جدًّا (١٠–١٥ كجم) باستخدام العُكَّازات أو المشاية. ويستمر هذا الأسلوب لمدة ٦–١٠ أسابيع، بهدف حماية منطقة المفصل المصاب أساسًا وليس المنطقة القصبية. ومن الأسبوع السادس إلى الأسبوع العاشر بعد الجراحة، يُحوَّل التحمّل الوزني الخفيف جدًّا تدريجيًّا إلى التحمّل الكامل للوزن خلال فترة تتراوح بين أسبوعين وثلاثة أسابيع. وبالمثل، ينبغي أن يحقّق المريض التحمّل الكامل للوزن دون الحاجة إلى أجهزة مساعدة (مثل العكّازات) بحلول الأسبوع الثاني عشر بعد الجراحة.
سابعًا: المتابعة
تقييم الجرح
يجب تقييم التئام الجرح بعد 2–3 أسابيع من العملية الجراحية. وبعد ذلك، عادةً ما يتم جدولة الزيارات المتابعة بعد 6 أسابيع و12 أسبوعًا و6 أشهر و12 شهرًا. وتسمح الصور الشعاعية المتسلسلة للجراح بتقييم تقدم التئام الكسر.
إزالة الغرسات
إزالة الغرسة ليست إلزامية، ولكن إذا ظهرت أعراض مرتبطة بالغرسة بعد اتحاد الكسر، فيجب مناقشة إزالتها مع المريض.
الوقاية من الجلطات الدموية والانسداد الوعائي
يجب أن تتبع الوقاية من الجلطات التوجيهات المؤسسية المحلية.