
Subtrochanteric Femur Fractures: Anatomy, Classification, and Treatment Options
Subtrochanteric (ST) femur fractures are defined as fractures occurring within 5 cm distal to the lesser trochanter. Overall, the estimated incidence of these fractures is approximately 15–20 per 100,000 people per year. The age distribution shows a bimodal pattern: individuals under 40 years account for about 20% of ST fractures, while those over 50 years account for more than two‑thirds. In younger populations, the male‑to‑female ratio is nearly equal; however, with increasing age, the incidence becomes higher in women. Additional risk factors for ST fractures include osteoporosis patients receiving bisphosphonate therapy, low total bone mineral density, and chronic conditions such as diabetes mellitus.
- Surgery is the mainstay of treatment for ST fractures, with intramedullary nails (IM) and extramedullary plates being the primary implants.
- Among these, intramedullary nailing offers biological and biomechanical advantages and has become the gold standard for treating ST femur fractures.
- Orthopaedic surgeons should be familiar with and proficient in multiple reduction techniques to achieve anatomic alignment in all unique ST fracture patterns.
- This article provides a comprehensive review of the epidemiology, anatomy, biomechanics, clinical presentation, diagnosis, and treatment of subtrochanteric femur fractures.
Anatomy
To properly diagnose and treat ST fractures, orthopaedic surgeons must have a thorough understanding of the relevant anatomy. The ST region includes the metaphyseal‑diaphyseal junction of the proximal femur within 5 cm distal to the lesser trochanter. The calcar femorale is crucial for maintaining the integrity of the proximal femoral bony structure, providing mechanical support to the proximal femur. This dense bony structure is located on the posteromedial aspect of the femur, arising distal to the lesser trochanter and coursing to terminate at the posterior‑inferior aspect of the femoral neck. During standing and walking, the calcar femorale may bear loads exceeding 1000 N. The ST region is also influenced by multiple muscle attachments. These muscles generate secondary forces that increase stresses across the proximal femur and hip. Relevant muscles include the hip abductors, adductors, short external rotators, and the iliopsoas.
Biomechanics
Multiple deforming forces act on the proximal and distal fracture fragments, leading to characteristic deformities. On the proximal fragment, the gluteus medius and minimus cause abduction, the iliopsoas causes flexion, and the short external rotators (piriformis, obturator internus, quadratus femoris, and the superior and inferior gemelli) cause external rotation. On the distal fragment, the gracilis and adductors produce adduction and shortening forces (Figure 1). Together, these forces result in the characteristic deformity of ST fractures: the proximal fragment is abducted, externally rotated, and flexed, while the distal fragment is adducted—overall producing a typical varus and procurvatum fracture pattern. These anatomic deforming forces make intraoperative reduction of ST fractures challenging.
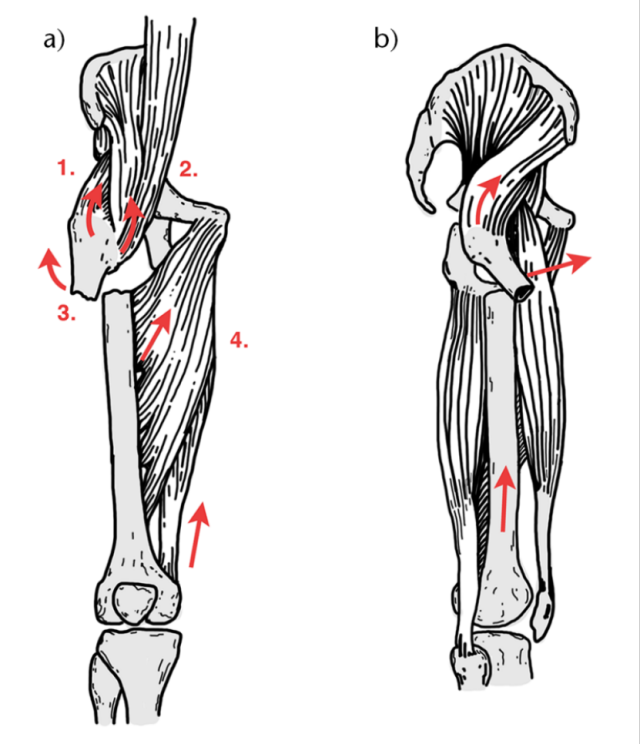
Figure 1: Deforming forces (red arrows) on the proximal and distal fragments in the coronal (A) and sagittal (B) planes of subtrochanteric fractures. The proximal fragment is abducted by the gluteus medius and minimus (1), flexed by the iliopsoas (2), and externally rotated by the short external rotators (3). The distal fragment is adducted and shortened by the adductors and gracilis (4).
Classification
Several classification systems exist for ST femur fractures. The Russell‑Taylor classification is based on involvement of the lesser trochanter and whether the fracture extends into the piriformis fossa. Prior to the development of trochanteric‑entry nails, this classification was used to distinguish fractures suitable for intramedullary nailing from those requiring lateral fixed‑angle devices. Russell‑Taylor type I fractures do not involve the piriformis fossa and can be treated with intramedullary nailing via a piriformis‑fossa entry.
Source: Rizkalla JM, Nimmons SJB, Jones AL. Classifications in Brief: The Russell‑Taylor Classification of Subtrochanteric Hip Fracture. Clin Orthop Relat Res. 2019 Jan;477(1):257‑261. doi: 10.1097/CORR.0000000000000505. PMID: 30586343; PMCID: PMC6345285.
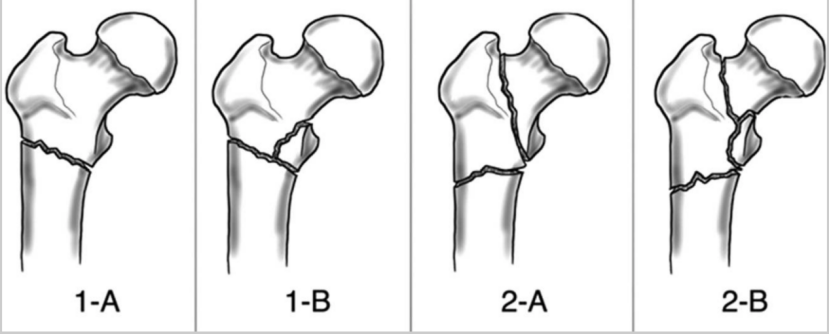
The figure depicts the four fracture types defined by the Russell‑Taylor classification system:
Type 1‑A: Fracture does not involve the piriformis fossa.
Type 1‑B: Fracture does not involve the piriformis fossa but involves the lesser trochanter.
Type 2‑A: Fracture traverses the piriformis fossa but does not involve the lesser trochanter.
Type 2‑B: Fracture involves both the lesser trochanter and the piriformis fossa.
The AO/OTA classification has the advantage of universality. It is worth noting that, to date, no single classification system appears to be ideal for guiding treatment, predicting prognosis, and achieving satisfactory interobserver reproducibility.
Two specific ST fracture patterns warrant recognition—reverse oblique fractures and atypical fractures.
Reverse oblique fractures are intertrochanteric or subtrochanteric (depending on the proximal extent of the fracture) injuries in which the main fracture line runs from proximal‑medial to distal‑lateral. These fractures have a tendency for medial shaft displacement, have a high implant failure rate when treated surgically with a sliding hip screw, and are best managed with intramedullary nailing.
Atypical fracture patterns are associated with bisphosphonate use. For atypical femoral fractures, it is important to identify the major underlying risk factors: these fractures have a relatively high rate of bilateral involvement; if an incomplete lesion of the lateral femoral cortex is present, prophylactic fixation should be performed to avoid progression to a complete fracture. It is recommended to discontinue bisphosphonates and switch to other agents. The American Society for Bone and Mineral Research has classified the common radiographic features of atypical ST fractures into major and minor criteria. Four of the five major criteria must be met to define a fracture as atypical, while minor criteria may be present or absent on an individual basis. Major criteria include: low‑energy trauma, minimal comminution, a transverse fracture originating from the lateral cortex, lateral cortical thickening, and a medial spike associated with a complete fracture.
Clinical Evaluation
The clinical presentation of patients with ST fractures shows a bimodal distribution. In younger patients, subtrochanteric fractures are typically caused by high‑energy trauma, such as motor vehicle collisions or falls from height. This injury mechanism is often associated with other traumatic injuries, and the patient should be comprehensively evaluated by the trauma team. In elderly patients, ST fractures are usually the result of low‑energy trauma and often present as isolated injuries. The surgeon should obtain a detailed history, assessing comorbid conditions and medication use, with particular attention to bisphosphonate regimens and duration of use.
Physical examination of the affected limb typically reveals shortening and external rotation. The patient complains of hip and/or thigh pain, inability to bear weight, and pain with hip motion. Although these fractures are usually closed injuries, a skin examination should be performed because the marked flexion of the proximal fragment may jeopardize the overlying skin. The physical examination should include assessment of the integrity of the surrounding neurovascular structures. A full skeletal survey should be performed to rule out associated orthopaedic injuries. After excluding other injuries to the ipsilateral lower extremity, the patient may be placed in traction, which can help restore fracture length and improve preoperative pain scores.
Imaging Evaluation
Appropriate imaging studies are essential for correctly identifying and classifying the fracture, providing the basis for preoperative planning. For patients with suspected ST fractures, initial imaging workup should include: anteroposterior (AP) pelvis, AP and lateral views of the femur, and AP and lateral views of the knee. Contralateral femoral imaging may be useful for assessing femoral anteversion. In comminuted fractures where cortical landmarks for anatomic reduction are absent, contralateral views are particularly helpful. CT scanning is not routinely required but is often performed as part of the initial trauma evaluation; CT images should be carefully reviewed. CT provides a more comprehensive assessment of fracture morphology, including the proximal extension of the fracture. This information influences preoperative planning, reduction methods, and implant selection. Classic radiographic findings of ST fractures include: abduction, external rotation, and flexion of the proximal fragment; and adduction of the distal fragment.
Treatment
Non‑operative management of ST fractures is generally not feasible. Without surgical reduction and fixation, patients have a high risk of malunion or nonunion; more importantly, patients are rendered non‑ambulatory, leading to increased mortality. The few patients who may be considered for non‑operative treatment include those who cannot tolerate surgery due to prohibitive anesthesia‑related risks, or those who are receiving hospice care with only mild hip symptoms. However, given that surgery provides pain relief and improved mobility, all members involved in the decision‑making process should carefully discuss non‑operative options before proceeding.
Surgical treatment of ST fractures can be broadly divided into two main categories: intramedullary nail (IM) fixation and extramedullary plate fixation (Figure 2; Table 1). Among these, intramedullary nailing has become the gold standard for treatment for multiple reasons—shorter hospital stays, less blood loss, shorter overall operative time, immediate weight‑bearing, and better functional outcomes. Data indicate that the vast majority of ST fractures are treated with intramedullary nails. Intramedullary nails also offer biomechanical advantages, with higher stiffness and strength and a shorter lever arm, meaning a stronger construct and less strain on the implant. Nail entry point and implant design influence fracture reduction and stability; therefore, surgeons should understand the modifiable factors that can improve outcomes.
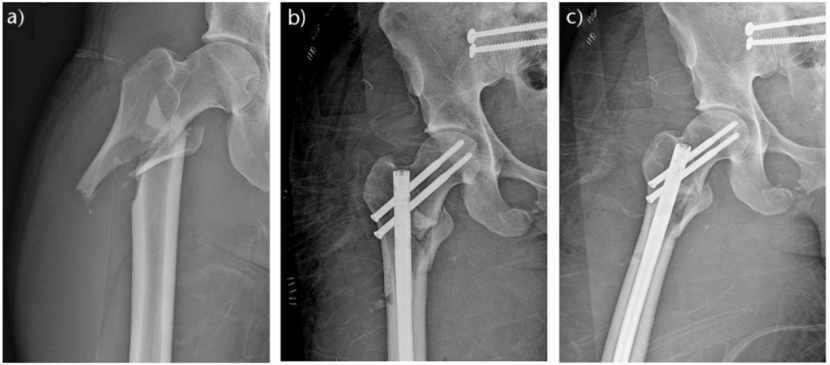
Figure 2: Radiographs of a right‑side subtrochanteric femur fracture (with intertrochanteric extension). A: Preoperative AP view. B: Immediate postoperative AP view. C: Immediate postoperative lateral view. This fracture was treated with a reconstruction intramedullary nail via a piriformis‑fossa entry.
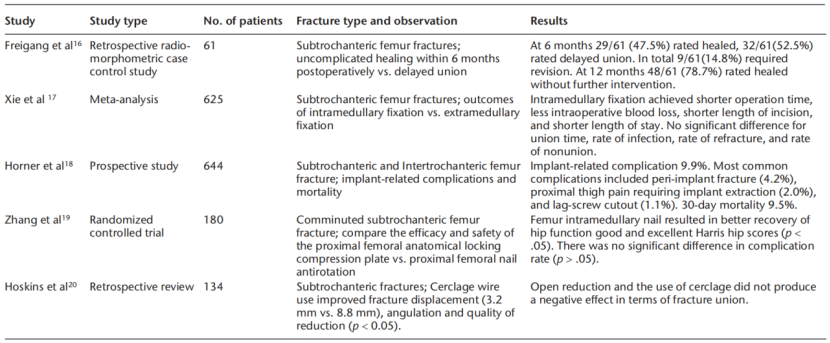
Table 1: Current evidence for subtrochanteric femur fractures (title only, no detailed contents provided in original).
Regarding the entry point, the surgeon may choose either the piriformis‑fossa or the trochanteric entry. For both approaches, the incision should be made proximal to and aligned with the axis of the medullary canal curvature of the femur, avoiding injury to the superior gluteal nerve. A more posterior incision allows the guide wire to be inserted from posterior to anterior, aligning with the anatomic curvature of the femur. This reduces the risk of eccentric reaming of the proximal fragment in the sagittal plane. The piriformis‑fossa entry has the advantage that a straight nail aligns with the coronal axis of the femoral medullary canal. This colinearity reduces the risk of varus malunion and also minimizes the risk of eccentric medial cortex reaming. However, the piriformis‑fossa approach is more challenging in obese patients. Excessive anterior placement increases the risk of anterior cortical perforation. The trochanteric entry is more superficial and may slightly reduce soft‑tissue dissection. However, it violates the abductor insertion. Additionally, the trochanteric entry carries a higher risk of varus malunion. Moreover, the significant anatomic variability of the trochanter among patients leads to high surgical variability. Overall, the choice of entry should be individualized, taking into account patient anatomy, surgeon preference, fracture characteristics, and the extent of the fracture pattern.
For treating ST fractures, the ideal intramedullary nail is an antegrade cephalomedullary nail. This nail requires static distal locking. It provides proximal fixation within the femoral neck and head. Options include a large cephalomedullary screw or a helical blade. However, these devices work primarily through fracture compression and are of greater utility in intertrochanteric fractures. Alternatively, two smaller‑diameter reconstruction screws may be used. This reduces bone removal within the femoral neck and head while still providing adequate proximal fixation. Other favorable nail features include a larger proximal diameter and the use of a full‑length nail. Compared to short nails, full‑length nails improve both rotational and axial stability. This enhances overall construct strength and also reduces the risk of postoperative periprosthetic fracture. The use of two distal interlocking screws provides stronger rotational and axial stability than a single screw.
The second major category of surgical fixation for ST fractures is the use of locking or fixed‑angle extramedullary plates. The implantation of fixed‑angle blade plates is technically demanding. This factor, combined with lower union rates, longer operative times, longer time to weight‑bearing, and higher infection rates compared to intramedullary nailing, has led to a decline in their use. Locking plates have demonstrated better biomechanical performance than fixed‑angle blade plates. However, studies by Collinge et al. have shown that these constructs led to fixation failure, malalignment/malunion, and deep infections in over 40% of patients; more than one‑third of these patients required revision surgery. Nonetheless, extramedullary plates still have a role, particularly when open reduction is required, using small‑fragment plates as temporary fixation. With this temporary plating technique, the malunion rate has been reduced from 27% to 0%.
Reduction Strategies and Techniques
Due to the deforming forces acting on ST fractures, a variety of techniques can be employed to achieve anatomic reduction. These reduction techniques include: use of reduction forceps, a ball‑spike pusher combined with a bone hook, percutaneous Schanz pins as joysticks, a femoral distractor, finger‑type reduction tools, blocking screws or wires, and cerclage wires. Preoperative patient positioning should incorporate the surgeon's habits and preferences, as each position has its advantages and disadvantages. For example, in the lateral decubitus position, adducting the affected limb can facilitate access in obese patients, and this position also makes reduction of the distal fragment easier. The supine position is familiar to most surgeons, offers advantages in polytrauma situations by allowing access to other limbs, and protects an injured spine.
For many ST fractures, reduction forceps can be considered to help maintain reduction (Figure 3). This technique yields good reduction results and high union rates. For simple two‑part ST fractures, percutaneous Schanz pins as joysticks, or a ball‑spike pusher combined with a bone hook, can be used to align the fragments and allow proper guide‑wire placement. Schanz pins can also be used in conjunction with a femoral distractor to first restore fracture length and then lock the reduction once satisfactory alignment is achieved.
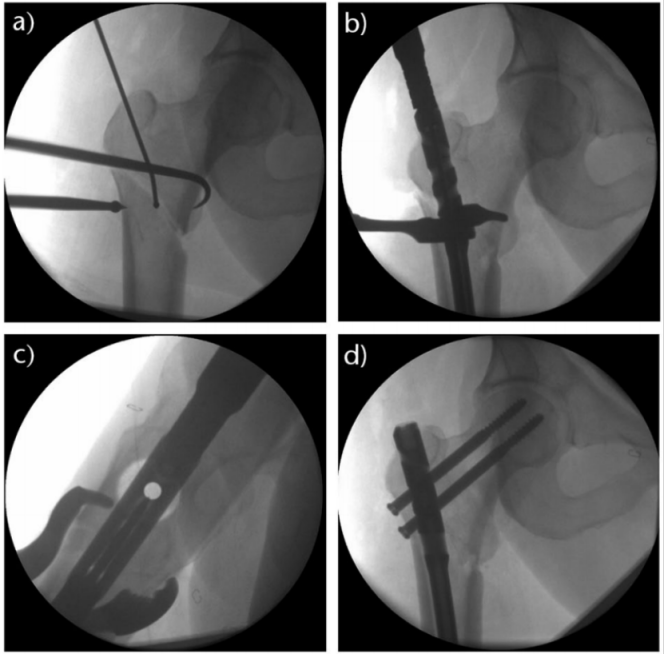
Figure 3: Use of a ball‑spike pusher to push the distal fragment medially while a bone hook retracts the proximal fragment to correct varus deformity (A). After guide‑wire placement, reduction forceps maintain the reduction in the coronal (B) and sagittal (C) planes. After anatomic reduction is achieved, the subtrochanteric fracture is fixed with a reconstruction intramedullary nail via a trochanteric entry (D).
For two‑part ST fractures, a finger‑type reduction tool is very useful (Figure 4). Longitudinal traction generally improves length, but because the abductors attach proximally and the adductors attach distally, varus malalignment often persists; the finger‑type tool can then control the proximal fragment to correct varus. Improper guide‑wire entry or trajectory can cause eccentric reaming, which may lead to cortical perforation or disrupt an already achieved reduction. For more complex fracture patterns (those with comminution or distal extension), blocking screws or wires can be placed on the concave side of the proximal fragment deformity to maintain reduction and enhance construct stiffness (Figure 5). Although there are concerns about compromising femoral blood supply, percutaneous cerclage wires have been shown to be an effective and safe method for reduction.
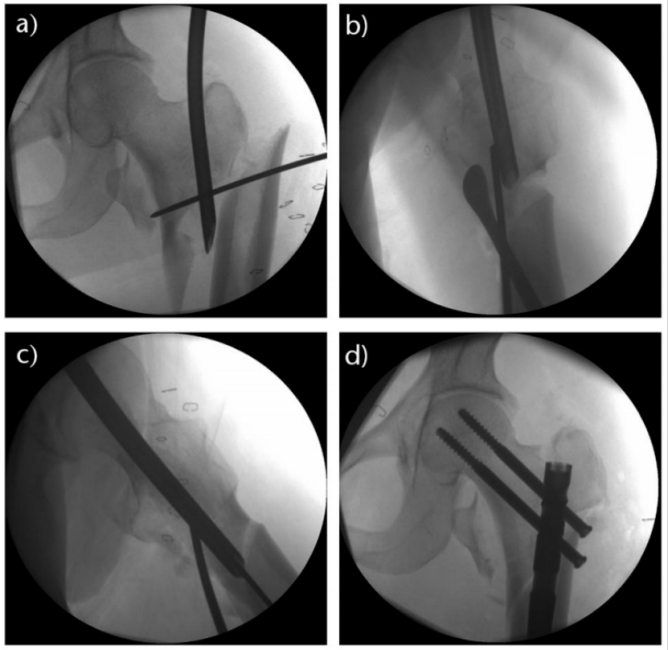
Figure 4: Multiple reduction techniques used for this complex subtrochanteric fracture with intertrochanteric extension. A finger‑type reduction tool is placed through a piriformis‑fossa entry to control the proximal fragment (A). A Cobb elevator and a posterior blocking wire are used to correct sagittal deformity (B). The finger‑type tool is then advanced to the level of the distal fragment to allow passage of the guide wire (C). After anatomic reduction is achieved, a piriformis‑fossa entry reconstruction intramedullary nail maintains the reduction (D).
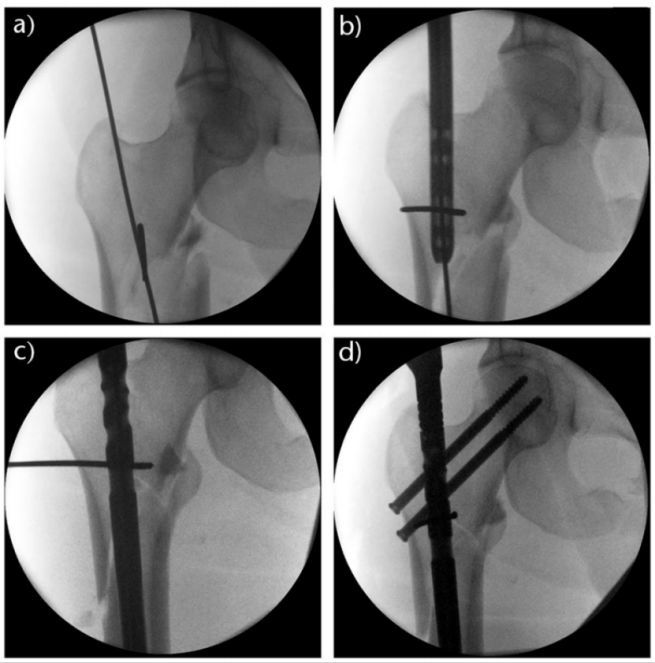
Figure 5: A blocking wire is placed on the concave side of the proximal fragment deformity, medial to the guide wire, and left in place during reaming to guide reaming of the proximal fragment (A). During nail insertion (B), the blocking wire effectively displaces the distal fragment laterally (C), thus achieving anatomic reduction, which is maintained with a piriformis‑fossa entry reconstruction intramedullary nail (D).
Complications
Surgical complications of ST fractures are similar to those of other proximal femoral fractures and include malunion, nonunion, infection, implant failure, and death. The 30‑day, 1‑year, and 4‑year mortality rates for ST fractures are approximately 9.5%, 27%, and 60%, respectively.
One of the most common complications following internal fixation of ST fractures is varus, procurvatum malunion or nonunion. This risk is primarily related to suboptimal intraoperative anatomic reduction; consistent use of proper reduction techniques should improve alignment and reduce healing‑related complications.
Malunion may also involve rotational deformity, which can lead to gait abnormalities and hip pain. Rotational malalignment is particularly common when a traction table is used, as excessive internal rotation is often employed to attempt fracture reduction. This is especially concerning in severely comminuted fractures. If the fracture heals in the typical ST malreduction pattern, excessive varus angulation and flexion of the proximal fragment will negatively alter the patient's gait mechanics. Symptomatic malunion may require osteotomy and internal fixation; nonunion can be effectively managed with implant exchange, with or without bone grafting. As with all surgeries, infection is a potential risk. Superficial infections can often be managed with antibiotics alone. However, deep infections require surgical irrigation and debridement, and may necessitate implant removal. In cases of infected nonunion, implant removal and exchange to an antibiotic‑loaded intramedullary implant, combined with long‑term intravenous or oral antibiotics, is required.
Conclusion
Subtrochanteric (ST) femur fractures are challenging. The deforming forces are large and complex, making reduction and fixation difficult. Surgery remains the definitive treatment for these fractures, and understanding these forces and the techniques for proper reduction is essential to improve alignment, stability, and patient outcomes.
References:
1. Subtrochanteric femur fractures: current review of management.
2. Classifications in Brief: The Russell‑Taylor Classification of Subtrochanteric Hip Fracture.